Introduction
Allergic diseases such as asthma, atopic dermatitis (AD), allergic rhinitis (AR), and urticaria impose a significant global health burden, affecting millions of individuals worldwide, with increasing prevalence and profound impacts on their quality of life [1]. The origins of these disorders are multifaceted and complex, with genetic predisposition, environmental influences, and disruptions in the immune system all playing crucial roles [2–4]. Within the array of factors that may contribute to the development of allergic diseases, early life events, including neonatal jaundice, have gained attention as potential risk factors for these conditions [5].
Neonatal jaundice, also known as hyperbilirubinemia, is a frequently encountered condition in newborns, characterized by high levels of bilirubin in the blood. This occurs because the liver of a newborn is not yet fully developed and therefore has a limited capacity to process and eliminate bilirubin, a yellow pigment that is a byproduct of the breakdown of red blood cells [6]. A growing body of observational research has noted an association between neonatal jaundice and an elevated risk of developing various allergic diseases, such as asthma [7], AD [5, 7, 8], AR [5, 7], urticaria [5], and allergic conjunctivitis (AC) [5]. However, these studies are not without their limitations. The potential for confounding factors and the issue of reverse causality pose significant challenges to establishing a definitive causal link.
To address the limitations inherent in observational studies, which are often subject to confounding factors and reverse causality, we employed Mendelian randomization (MR), a method that leverages genetic variants as instrumental variables (IVs) to estimate causal effects. This approach is particularly effective in minimizing the impact of confounding factors [9, 10]. For instance, numerous studies across various fields have demonstrated the utility of MR in elucidating causal pathways in epidemiological research [11–13]. Our study used MR to assess whether neonatal jaundice causally increases the risk of allergic diseases. Establishing such a causal relationship is crucial, as it could provide valuable insights into the etiology of allergic disorders and help identify potential targets for prevention and intervention strategies. The findings of this study could have significant implications for public health policies and clinical practice related to the management of neonatal jaundice and the prevention of allergic diseases, potentially leading to more effective interventions and improved outcomes for affected individuals.
Material and methods
Study design
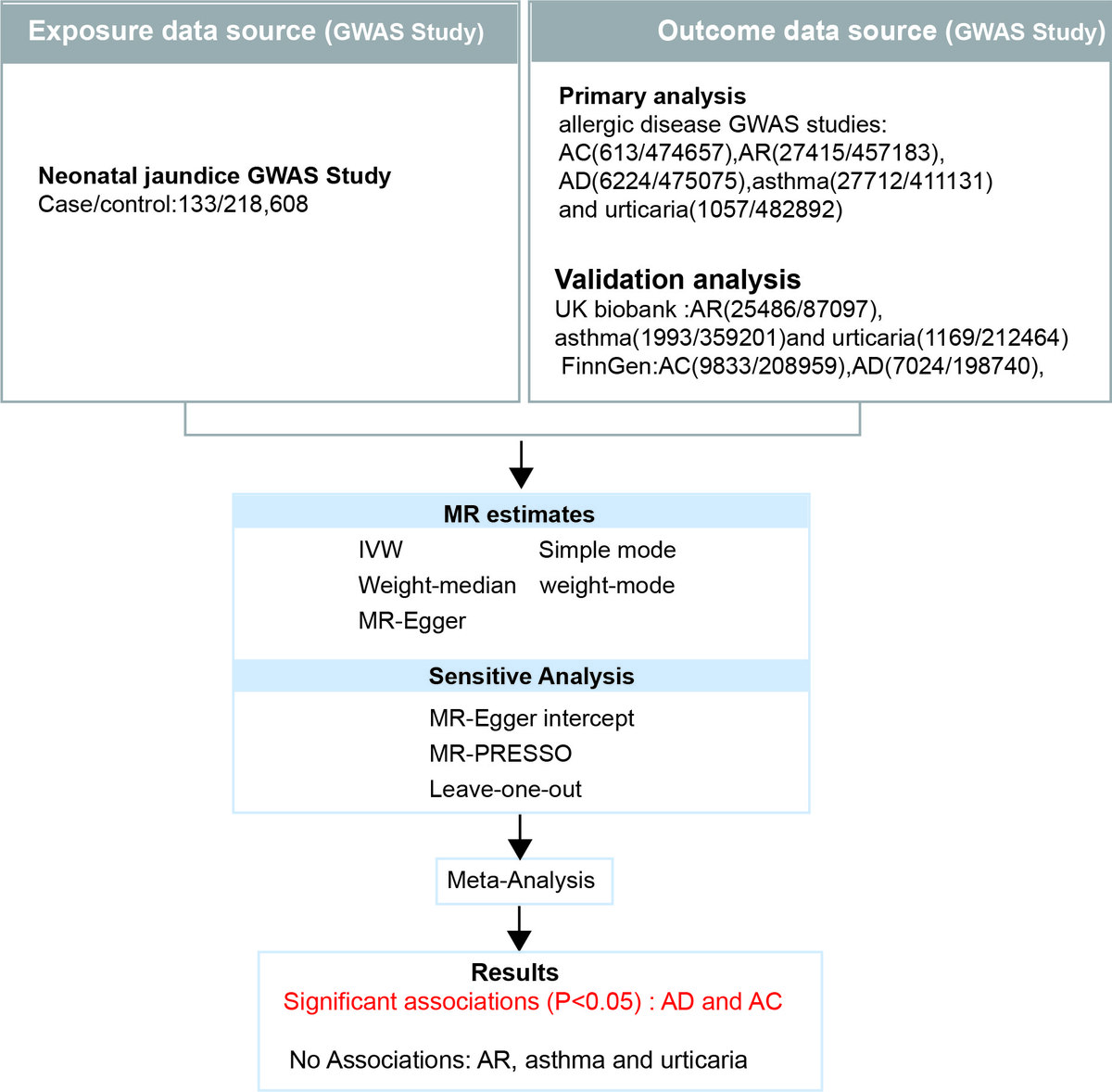
Figure 1 presents the study design for our MR analysis. The study is based on three key assumptions [14]. Firstly, the genetic variants used as IVs are strongly correlated with neonatal jaundice exposure. To assess the strength of these associations and reduce the potential for weak instrument bias, we employed the F-statistic. A threshold F-value of 10 was used, as values above this threshold suggest that the instruments are strong, meaning they have a robust association with the exposure (neonatal jaundice). Secondly, the genetic variants influence the allergic disease outcome only through their effect on neonatal jaundice exposure, without any direct effect on the outcome itself. This assumption is crucial for ensuring that the IVs satisfy the exclusion restriction condition of MR analysis. Thirdly, the IVs were assumed to be free from confounding factors, meaning they should not be associated with any other factors that affect the allergic disease outcome. This assumption was based on the rigorous selection criteria for single-nucleotide polymorphisms (SNPs, discussed below) and the use of large-scale datasets with well-characterized exposure and outcome measures.
Figure 1
Overview of study design
GWAS – genome-wide association studies, MR – Mendelian randomization, AC – allergic conjunctivitis, AR – allergic rhinitis, AD – atopic dermatitis, SNPs – single nucleotide polymorphisms, IV – instrumental variable, IVW – inverse variance weighted.
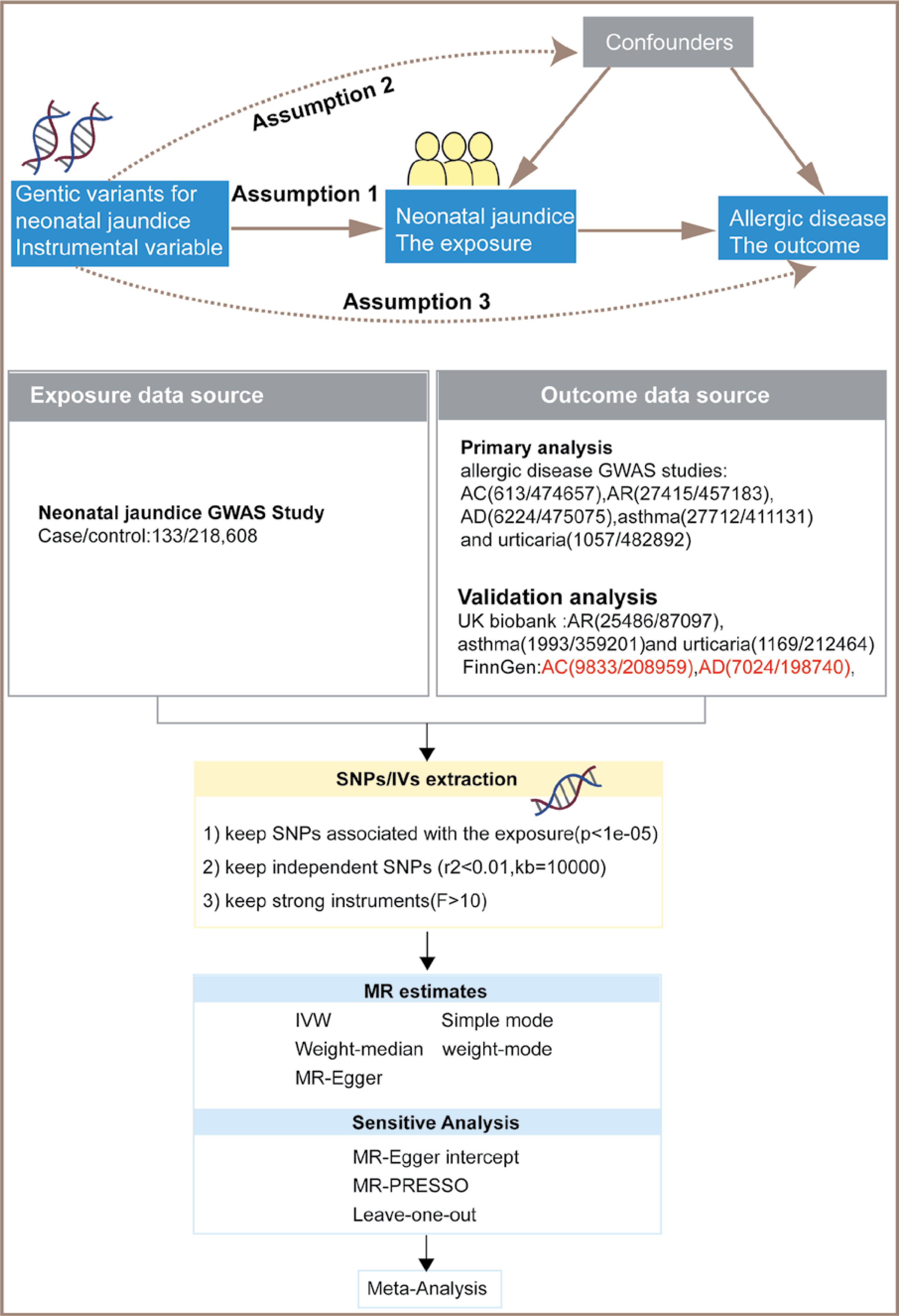
The preprocessed neonatal jaundice exposure data were analyzed using MR in conjunction with allergic disease outcome data from two separate databases. Subsequently, a meta-analysis was conducted on the instrumental variable weight (IVW) results from the MR analyses of allergic disease data across different databases, with multiple adjustments made to the meta-analysis results to ensure data integrity. The integration of MR analysis with meta-analysis provides a unique advantage by aggregating data from numerous studies, which can help mitigate bias, dissect heterogeneity, and broaden the scope of generalizability. This combined approach allows for a more comprehensive evaluation of the relationship between exposure and outcome, leading to more robust findings and a deeper exploration of the research hypothesis. The MR analysis used publicly available data from large-scale consortia and cohort studies. Ethical consent and approval were not required for this study, as the constituent studies had already obtained approvals from their respective institutional review boards or ethics committees.
Selection of instrumental variables
To ensure the validity of the MR analysis, we followed the recommendations of Zhu et al. [15] by selecting at least 10 independent SNPs as IVs for neonatal jaundice.
The selection process involved the following key criteria:
Firstly, SNP selection based on statistical association with neonatal jaundice: We identified SNPs that were significantly associated with neonatal jaundice exposure through a pooled genome-wide association study (GWAS) dataset [16]. The p-value threshold for selecting SNPs was set to 1 × 10–5, a commonly used threshold in MR studies [17], to ensure sufficient statistical power and a sufficient number of genetic variants for robust analysis.
Secondly, to minimize the risk of confounding due to linkage disequilibrium (LD) between SNPs, we ensured the independence of selected SNPs. According to Purcell et al. [18] and Barrett et al. [19], SNPs were considered independent if their linkage disequilibrium coefficient (r2) was less than 0.01, which corresponds to a minimal level of correlation between them. This threshold was chosen to ensure that the genetic variants used as IVs represent distinct genetic loci, thus reducing potential bias from pleiotropy (where a single SNP affects multiple traits) [20].
Thirdly, to further minimize potential biases from genetic pleiotropy and ensure the independence of SNPs, we defined the linkage disequilibrium region width to be 10,000 kb (10 Mb). This width is commonly used in MR studies and is considered appropriate for ensuring that SNPs are sufficiently distant from each other to be considered independent [21, 22].
By applying these selection criteria, we aimed to choose a set of SNPs that are robustly associated with neonatal jaundice, independent from each other, and not influenced by confounding factors. This careful selection of IVs is fundamental to the validity of the MR analysis and the reliability of our conclusions regarding the causal relationship between neonatal jaundice and allergic diseases.
Genetic association data on neonatal jaundice
We sourced the genotypic and phenotypic association data from GWAS. The most recent and extensive GWAS summary data on neonatal jaundice were obtained from the IEU OpenGWAS project (available at mrcieu.ac.uk). The dataset included 133 cases and 218,608 controls, and the data were made accessible via the ‘GWAS ID’ (detailed in Supplementary Table SI). The study population comprised individuals of European descent.
Genetic association datasets for five common allergic diseases
We aimed to investigate the causal relationship between neonatal jaundice and five common allergic diseases: pediatric asthma, AD, AC, AR, and urticaria. To obtain comprehensive and current information on these outcomes in European populations, we selected the most extensive and recent GWAS studies for our preliminary MR analysis (details in Supplementary Table SI). The latest GWAS summary statistics for these diseases were retrieved from the European Bioinformatics Institute (EBI) database, a globally renowned, interdisciplinary, and publicly accessible repository in life sciences [23]. The outcome data comprised AC (613 cases and 474,657 controls), AR (27,415 cases and 457,183 controls), AD (6,224 cases and 475,075 controls), asthma (27,712 cases and 411,131 controls), and urticaria (1,057 cases and 482,892 controls). The study population consisted exclusively of individuals of European descent. To validate our findings, we used five key statistical measures on allergic disorders from the UK Biobank or FinnGen (validation details in Supplementary Table SI).
Statistical analysis
The inverse-variance weighted (IVW) method served as the primary approach for estimating causal effects in this study. Cochran’s Q test was employed to assess the heterogeneity of the impact of IVs on allergic diseases, with statistical significance set at p < 0.05. IVW random effects models were applied to infer causation in the presence of heterogeneity, while IVW fixed effects models were used when heterogeneity was absent [24]. Additionally, MR-Egger regression, weighted median, simple mode, and weighted mode were employed for MR analysis to estimate causal effects accurately. Fixed-effects meta-analysis was used to combine MR estimates for each outcome from different sources. The I2 statistic was used to evaluate the heterogeneity of outcomes from various data sources, with I2 values below 25%, between 25% and 75%, and above 75% indicating low, moderate, and high heterogeneity, respectively.
We used MR-PRESSO (Mendelian Randomization Pleiotropy RESidual Sum and Outlier) analysis and MR-Egger regression to assess the potential horizontal pleiotropy of the IV SNPs. MR-PRESSO analysis, with a global test p-value less than 0.05, identified outliers with horizontal pleiotropy. Similarly, MR-Egger regression with a p-value less than 0.05 confirmed the presence of horizontal pleiotropy [25]. After sequentially removing each SNP, the leave-one-out method was applied to recompute the overall association. Statistical analyses were conducted using R version 4.3.2, with the packages “TwoSampleMR,” “MR-PRESSO,” and “Meta.”
Results
Instrumental variables for neonatal jaundice
The summary statistics for the genetic IVs associated with neonatal jaundice are presented in Supplementary Tables SII–SIII. The F-statistics for these variables exceeded 20, indicating a lack of substantial evidence for weak instrument bias (Supplementary Tables SII–SIII). The specific SNPs used as IVs are detailed in Supplementary Tables SII–SIII.
Causal effect of neonatal jaundice on allergic diseases
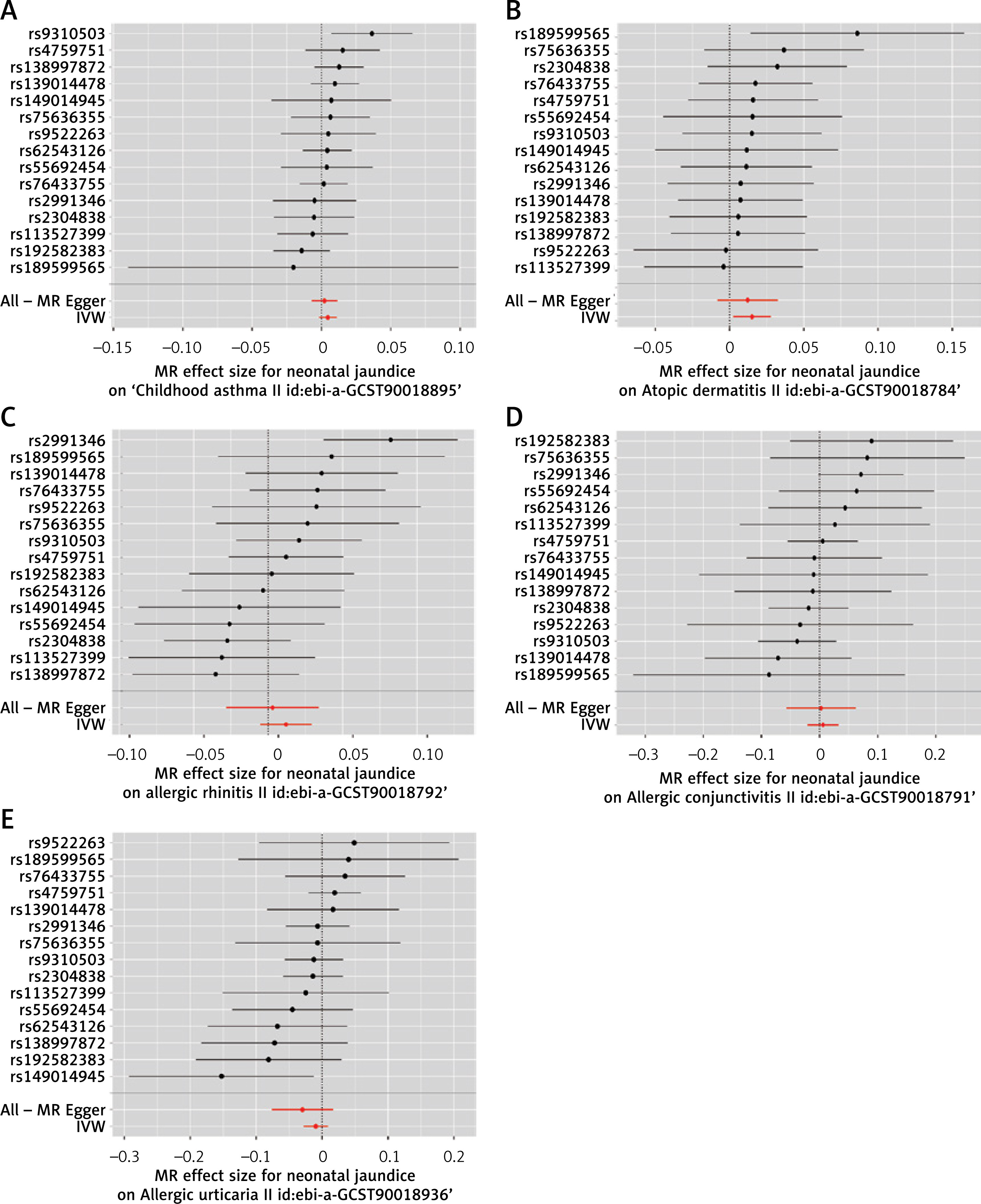
We employed the IVW method as the primary approach to assess the causal relationship between neonatal jaundice and allergic diseases. The MR analysis based on the IVW method revealed a significant association between genetically determined neonatal jaundice and AD (odds ratio (OR) = 1.0115, 95% confidence interval (CI) 1.0025-1.0282, p = 0.019) (Supplementary Tables SIV). The forest plots for this analysis are presented in Figure 2. However, neonatal jaundice was not significantly correlated with pediatric asthma, AR, AC, or urticaria (Figure 2). The weighted median and MR-Egger methods yielded similar results (Supplementary Figure S1, Supplementary Tables SIV), and the scatter plot is shown in Supplementary Figure S1.
Figure 2
A–E – Forest plot of SNPs associated with neonatal jaundice and their estimated associations with allergic diseases in EBI: A – association of neonatal jaundice with pediatric asthma; B – association of neonatal jaundice with atopic dermatitis; C – association of neonatal jaundice with allergic rhinitis; D – association of neonatal jaundice with allergic conjunctivitis; E – association of neonatal jaundice with allergic urticaria
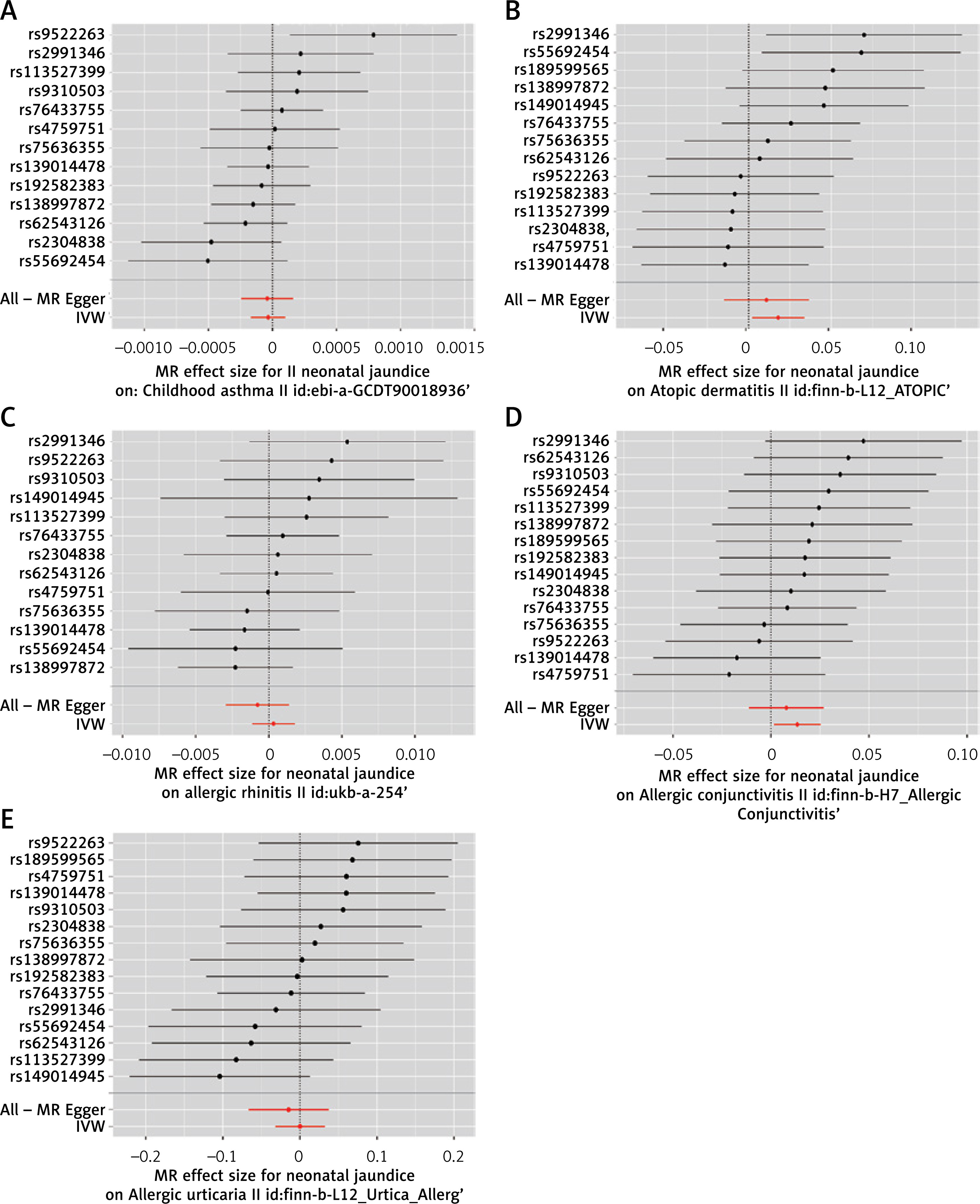
To ensure the consistency of our findings across different databases, we replicated the MR analysis using data from the UK Biobank (UKB) database or the FinnGen biospecimen database. This replication confirmed a similar causal association between neonatal jaundice and AD (UKB: OR = 1.0180, 95% CI: 1.0021–1.0341, p = 0.026) and a causal association with AC in the UKB cohort (OR = 1.0135, 95% CI: 1.0016–1.0255, p = 0.026), and the forest plots are shown in Figure 3. As expected, no causal association was found between neonatal jaundice and other allergic conditions, including pediatric asthma, AR, and urticaria (Supplementary Tables SV, Supplementary Figure S2).
Figure 3
A–E – Forest plot of SNPs associated with neonatal jaundice and their estimated associations with allergic diseases in FinnGen or UKB: A – association of neonatal jaundice with pediatric asthma; B – association of neonatal jaundice with atopic dermatitis; C – association of neonatal jaundice with allergic rhinitis; D – association of neonatal jaundice with allergic conjunctivitis; E – association of neonatal jaundice with allergic urticaria
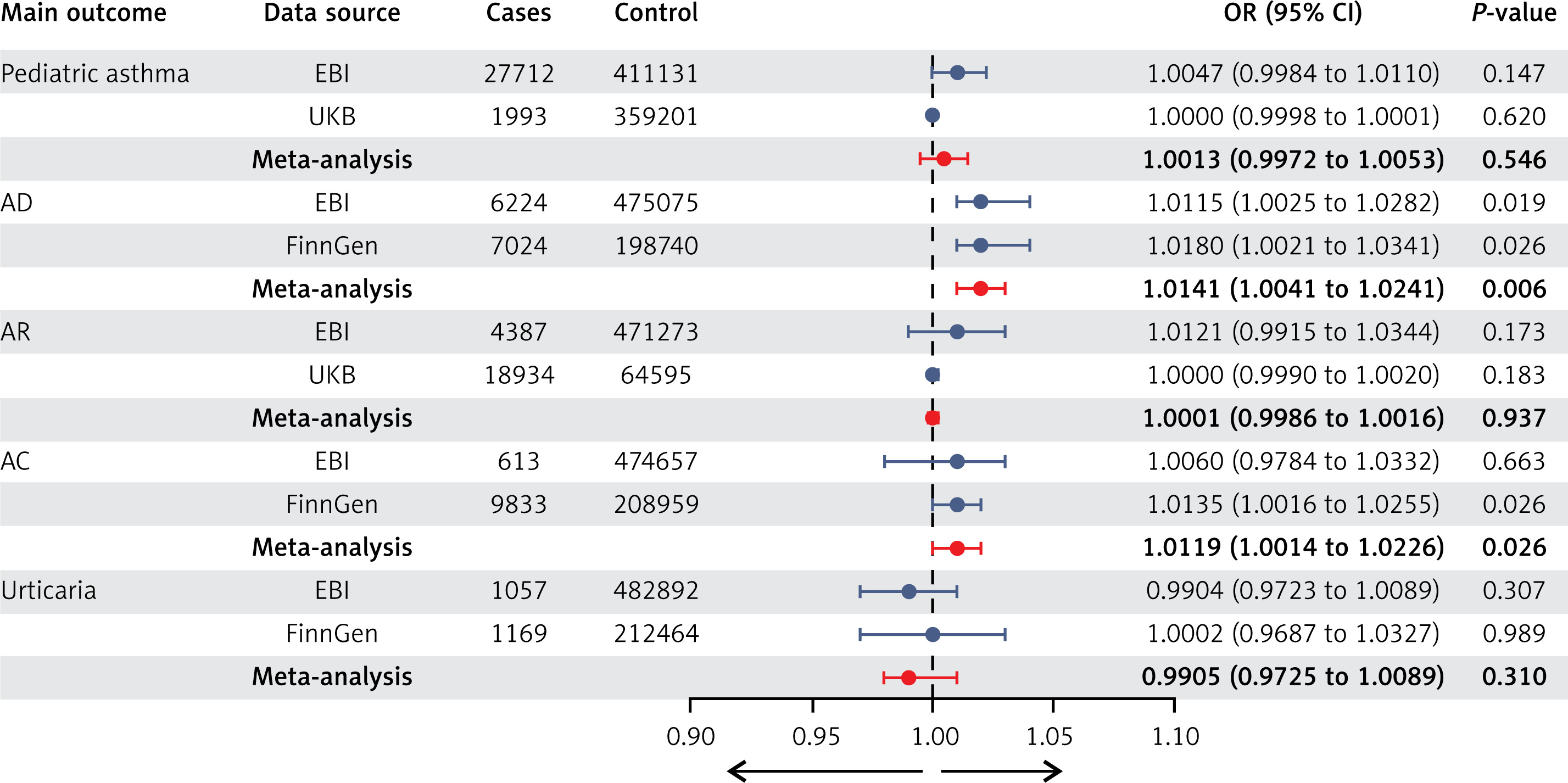
Furthermore, we combined MR estimates for each outcome from different sources using meta-analytic methods. The meta-analysis of IVW estimates indicated that neonatal jaundice was causally associated with allergic diseases. Specifically, neonatal jaundice was significantly associated with an increased risk of AD and AC (AD: OR = 1.0141, 95% CI: 1.0041–1.0241, p = 0.006; AC: OR = 1.0119, 95% CI: 1.0014–1.0226, p = 0.026). Conversely, neonatal jaundice was not significantly associated with pediatric asthma, AR, and urticaria. The weighted median and MR-Egger methods also produced similar results (Figure 4, Supplementary Tables SVI).
Figure 4
Meta-analysis depicting the association between genetically predicted neonatal jaundice and allergic diseases from two sources
Additionally, regarding the potential sample overlap issue, our analysis using an online platform (https://sb452.shinyapps.io/overlap/) showed that the proportion of overlapping participants between neonatal jaundice and the risk of AD, AC, and urticaria was below 0.35. Specifically, the overlap was 0.315 for AD, 0.318 for AC, and 0.314 for urticaria. This suggests that the overlap between the samples was minimal, with no significant impact on the results.
Sensitivity analysis of MR
To assess the heterogeneity among the neonatal jaundice and allergic diseases, we conducted Cochran’s Q tests for each dataset. The results revealed no significant heterogeneity for any of the datasets, with all p-values exceeding 0.05 (detailed in Supplementary Tables SVII, SVIII). These findings supported the use of the fixed-effects IVW approach as our primary analytical method.
We also examined the MR Egger regression intercepts for each dataset to assess for horizontal pleiotropy. No evidence of horizontal pleiotropy was detected, as the intercepts were close to zero, with non-significant p-values (detailed in Supplementary Tables SIX, SX), indicating that our results are unlikely to be biased by unmeasured confounding.
The MR-PRESSO global test did not identify any outlier SNPs or evidence of horizontal pleiotropy for neonatal jaundice in relation to allergic diseases across all datasets (detailed in Supplementary Tables SIX, SX). This further suggests that our analysis is robust against confounding bias.
In addition to these tests, we conducted sensitivity analyses using the leave-one-out method, which involved sequentially removing each SNP and recalculating the causal effects with the remaining SNPs. This approach confirmed the stability of our results, with minimal variation observed upon the removal of each SNP (Supplementary Figure S3). Moreover, volcano plots were generated to visually represent the heterogeneity across SNPs for each dataset (Supplementary Figure S4), providing a comprehensive assessment of the data consistency.
Discussion
Employing a combined approach of MR and meta-analysis, our study underwent a stringent screening and correction process, yielding robust results. Our findings suggest a causal association between neonatal jaundice and AD as well as AC. In contrast, no evidence was found to support a causal association between neonatal jaundice and childhood asthma, urticaria, or AR. The robustness of these findings was corroborated through sensitivity analyses, which included the Cochran’s Q, MR-Egger intercepts, MR-PRESSO, and leave-one-out methods. These findings not only fill a gap in the existing literature but also contribute to a deeper understanding of the impact of neonatal jaundice on allergic diseases.
Despite extensive research on the association between neonatal jaundice and allergic diseases [7, 26], there are limited studies that have revealed the actual effects of neonatal jaundice on allergic diseases due to the potential influence of confounding factors and reverse causality. Fortunately, MR is well suited to leverage publicly available data from large-scale GWAS to investigate the causal relationship between a genetically determined “exposure” and an “outcome,” while mitigating the inherent limitations associated with observational studies.
Consistent with our findings, a previous systematic review and meta-analysis showed that neonatal jaundice contributes to AD and AC [7, 26]. In a retrospective study by Egeberg et al. [8] involving 31,780 neonatally jaundiced infants and 641,834 controls, children with neonatal jaundice were at a slightly increased risk of AD compared to the reference population group (incidence rate ratio 1.13, 95% CI: 1.06–1.21). Additionally, a study by Apfelbacher et al. [27] identified a significant positive association between eczema and postnatal jaundice (OR = 1.27, 95% CI: 1.04–1.54). Furthermore, a retrospective cohort study by Wei et al. [5] found that the incidence rates and hazard ratios for five allergic diseases were significantly higher in the neonatal jaundice cohort compared to the non-neonatal jaundice cohort, with a hazard ratio of 2.51 (95% CI: 2.40–2.62) for AD. Even though several observational studies [28–32] have reported a significant association between neonatal jaundice and the incidence of childhood asthma, AR, or urticaria, our study found no significant association between neonatal jaundice and the risk of childhood asthma, AR, or urticaria. This finding is somewhat inconsistent with many published studies, which may be due to confounding factors such as delivery mode, birth weight, maternal exposure during pregnancy, education level, socioeconomic status, life habits, and selection bias.
Under the assumptions of MR, our findings suggest a causal association between neonatal jaundice and an increased risk of AD and AC. The precise mechanisms driving these causal effects are not yet fully understood, but several hypotheses have been proposed to explain the observed correlations. Current research suggests that bilirubin, a component of neonatal jaundice, may play a pivotal role in immune system development. Generally, the neonatal immune system tends to favor a Th-2 allergic/atopic sensitization response after birth, with an expected rapid transition to a Th-1 response [33]. However, experimental evidence indicates that the accumulation of intracellular unbound bilirubin might inhibit interleukin-2 (IL-2) production, thereby delaying the shift from Th-2 to Th-1 immune responses [34]. Additionally, the reduction in IL-6 levels, which also play a role in modulating immune responses, could further complicate this transition [35].
Although bilirubin is generally recognized as an antioxidant [36], its protective effects may be diminished in preterm infants [37]. Critically, at levels exceeding 12.5 mg/dl, bilirubin can transform into a potent oxidant, exerting pro-oxidant effects that may trigger inflammatory responses [38]. During episodes of neonatal hyperbilirubinemia, this oxidative stress could activate inflammatory pathways, potentially contributing to the development of allergic diseases later in childhood through alterations in the cytokine profile, such as increased TNF-α, IL-1β, and IL8 [35, 39].
Moreover, hyperbilirubinemia may compromise the integrity and maintenance of the skin barrier, rendering individuals more vulnerable to allergens and irritants. The disruption of this barrier can amplify immune responses, thereby facilitating the onset of AD [40].
Emerging evidence suggests that dysbiosis of the gut microbiota may contribute to both neonatal jaundice and atopic diseases. Studies have demonstrated that specific bacteria, such as Clostridium perfringens and Clostridium difficile, may promote the excretion of fecal urobilinoids, potentially contributing to the development of neonatal jaundice [41]. Additionally, the integrated analysis of microbiota with bile acids for the phototherapeutic treatment of neonatal jaundice highlights the complex interplay between gut microbiota and bile acid metabolism in this condition [42]. Alterations in gut bacterial flora have been implicated in the pathogenesis of atopic diseases [43, 44]. For instance, a clinical study on the prevention of AD by oral administration of probiotics in infants suggested that early intervention with probiotics may alter the risk of developing atopic diseases [45]. The gut microbiota plays a pivotal role in shaping the immune system, and dysbiosis could lead to an imbalance in immune responses, which may contribute to the development of AD and AC.
Genetic factors associated with neonatal jaundice, such as polymorphisms in glutathione S-transferase genes, may also play a role in the susceptibility to atopic diseases [46, 47]. These genetic variations may influence the body’s ability to process bilirubin and modulate immune responses, thereby contributing to the risk of developing atopic diseases.
The lack of association between neonatal jaundice and other allergic diseases, such as pediatric asthma, urticaria, and AR, may be attributed to differences in their pathophysiology. While AD and AC primarily involve skin-related immune responses, asthma, urticaria, and AR involve distinct pathways, including respiratory and systemic immune responses [28]. The specific mechanisms by which neonatal jaundice affects the development of these diseases warrant further investigation.
To visually represent the hypothesized pathways, we have included a conceptual diagram (Supplementary Figure S5) that outlines the complex biological interactions from elevated bilirubin levels to the development of AD and AC. This diagram highlights the interplay between bilirubin, cytokine profiles, skin barrier integrity, gut microbiota, and genetic factors in the context of immune system dysregulation, reinforcing the discussion on the proposed immunological mechanisms.
While our findings suggest a causal link between neonatal jaundice and the increased risk of AD and AC, the exact mechanisms remain to be fully elucidated. Future research should aim to clarify the role of unconjugated bilirubin, gut microbiota dysbiosis, skin barrier dysfunction, and genetic factors in the pathogenesis of atopic diseases. Additionally, studies examining the differential effects of neonatal jaundice on various allergic diseases could provide valuable insights into the complex interplay between jaundice and the immune system.
We performed rigorous selection of IVs for a two-sample MR analysis to investigate the association between neonatal jaundice and allergic diseases, reinforcing our findings with a meta-analysis of two datasets. This approach minimized confounding and reverse causality, ensuring robust results.
However, it is important to acknowledge that our study may not have fully accounted for potential confounders such as parental health conditions, which could influence both the incidence of neonatal jaundice and the risk of developing allergic diseases. For instance, parental allergies or chronic illnesses might affect the fetal environment and subsequent immune development. Moreover, the stringent experimental protocols employed in our analysis may have inadvertently overlooked certain associations. Our findings, based on European GWAS data, may not be generalizable to other racial and ethnic groups due to genetic and environmental differences. The limitations of GWAS, such as the absence of granular information on neonatal jaundice severity and the inability to capture rare genetic variants, also pose challenges.
Despite the capacity of MR analysis to address confounding, unmeasured factors such as socioeconomic status, parental allergies, and environmental allergen exposure could still have impacted the observed associations. Consequently, future research is imperative to corroborate our findings across diverse populations and with comprehensive data on potential confounders, thereby strengthening the causal inference.
Future research should incorporate parental health history, prospective cohort studies, and multivariable analyses to control for potential confounders. Additionally, future research directions should explore additional genetic factors and environmental interactions that may influence the development of allergic diseases in neonates with jaundice. This could involve GWAS with more diverse populations, as well as MR studies that can assess the causal role of specific genetic variants associated with both jaundice and atopy. To reinforce the findings and broaden their applicability across diverse populations, it will be crucial to conduct studies that include a wider range of genetic backgrounds and environmental contexts. This will help to determine whether the observed associations are consistent across different racial and ethnic groups and whether there are specific genetic or environmental factors that modify the risk of allergic diseases in the context of neonatal jaundice.
In conclusion, our study, using MR and meta-analysis of genetic data, strongly suggests a causal association between neonatal jaundice and elevated risks of AD and AC. In contrast, we found no evidence of a causal association between neonatal jaundice and childhood asthma, urticaria, or AR.
These findings have important implications for neonatal jaundice management and allergic disease prevention. Preventing or lessening neonatal jaundice may lower future risks of AD and AC. This discovery opens up new perspectives for understanding and managing allergic conditions, offering potential recommendations for the well-being of individuals with allergic conditions.