Introduction
Respiratory diseases represent a major global public health challenge and rank among the leading causes of mortality in adolescents and young adults (AYAs) [1]. Although their incidence in AYAs is lower than in older adults [2, 3], affected individuals in this age group have distinct biological, epidemiological, and clinical characteristics that differ from those of other age groups [4, 5]. These characteristics, combined with the fact that AYAs are at a critical stage of life for education, career establishment, and family formation, mean that respiratory diseases in this population can lead to disproportionate social and economic consequences, including work absenteeism, financial strain, and academic disruptions due to frequent healthcare use [6, 7]. Therefore, improving clinical recognition of respiratory disease burden in AYAs and developing evidence-based interventions targeting modifiable risk factors are critical for better health outcomes in this vulnerable population.
Globally, the burden of respiratory diseases among AYAs varies substantially by region [8]. Epidemiological data show that lower respiratory infections in individuals aged 15–49 years have an incidence rate of 2249.6 and a mortality rate of 4.1 per 100,000 population [3]. Similarly, European Union data reported a mortality rate of 0.62 per 100,000 population for chronic respiratory diseases among 10–24-year-olds in 2019. Previous GBD-based studies have examined specific respiratory conditions, such as the increasing burden of tracheal, bronchial, and lung (TBL) cancer attributable to ambient particulate matter pollution and smoking across all age groups and regions [9]. However, these analyses have primarily focused on the general population, leaving the AYA group largely undercharacterized. Therefore, this study provides the first comprehensive assessment focused specifically on respiratory diseases in AYAs, with detailed stratification and systematic evaluation of attributable risk factors.
This study aimed to evaluate the global burden of respiratory diseases and their attributable risk factors from 1990 to 2021 in AYAs, examining temporal trends, quantifying the contribution of major risk factors, and assessing disparities by age, sex, geographic location, and sociodemographic index (SDI). By elucidating these disparities, our findings can inform targeted respiratory disease control strategies, address health inequities, and optimize resource allocation for this priority population.
Material and methods
Data sources
This study used data from the Global Burden of Disease Study (GBD) 2021, which provides comprehensive estimates for 369 diseases and injuries, 88 risk factors, and related health metrics across 204 countries and territories from 1990 to 2021. Data came from multiple sources, including nationally representative household surveys, health examination surveys, population censuses, remote-sensing data, and administrative records [10]. For this analysis, we extracted country-level estimates for all 204 countries and territories using the GBD Results Tool, which provides pre-aggregated estimates at national, regional, and global levels with associated uncertainty intervals. Data were downloaded as CSV files for the specific causes, risk factors, age groups, and years of interest, following the standard GBD data extraction protocol [11]. We specifically focused on respiratory diseases with onset during AYAs (ages 15–39 years) [12], examining age-specific, sex-specific, and region-specific estimates of incidence, mortality, disability-adjusted life years (DALYs) and attributable risk factors. All data were extracted from the publicly available GBD 2021 database (https://ghdx.healthdata.org/gbd-2021).
Case definitions
Respiratory diseases were classified according to the standardized GBD 2021 framework, including: chronic obstructive pulmonary disease (COPD), asthma, pneumoconiosis, interstitial lung disease and pulmonary sarcoidosis (ILD/PS), upper respiratory infections (URIs), lower respiratory infections (LRIs), tracheal/bronchus/lung (TBL) cancers, pulmonary arterial hypertension (PAH), and tuberculosis (TB). Case definitions were based on the International Classification of Diseases (ICD) system, with detailed mappings to both ICD-10 and ICD-9 codes provided in Supplementary Table SI. Other respiratory conditions captured in GBD (e.g., COVID-19, otitis media, and rare chronic respiratory diseases) were excluded due to the study period, disease classification, or negligible burden in the AYA population.
Risk factor attribution
Risk factor estimation followed established GBD methodologies as previously described [11]. We included only risk-outcome pairs with convincing or probable evidence of causal relationships based on systematic reviews of epidemiological evidence. For each risk factor, exposure distributions were estimated using all available data sources, including population surveys and environmental monitoring data. Theoretical minimum risk exposure levels were determined based on current scientific evidence. Population attributable fractions (PAFs) [13] were calculated by comparing current exposure levels to these theoretical minimums, then multiplied by disease-specific burden estimates to determine attributable DALYs and deaths for each risk factor. All estimates were stratified by age, year, sex, location and SDI.
For this analysis, we included all risk factors associated with each respiratory disease outcome as defined in the GBD 2021 framework, encompassing both Level 2 and Level 3 risk factors. Specifically, we incorporated the complete set of GBD-established risk-outcome pairs for COPD, asthma, pneumoconiosis, LRIs, TBL cancers, and TB. These risk factors span multiple categories, including air pollution, smoking, occupational exposures, metabolic factors (high BMI, high fasting plasma glucose), dietary factors, alcohol use, physical inactivity, environmental exposures (residential radon), and others such as non-optimal temperature. A complete list of all risk factors analyzed for each disease outcome, including GBD risk factor IDs and definitions, is provided in Table I.
Table I
Global burden of deaths and DALYs from respiratory diseases attributed to risk factors in adolescents and young adults in both sexes combined, with percent change
Statistical analysis
Age-standardized rates (ASRs) were calculated using the GBD global reference population to enable comparison across populations with different age structures [14]. We reported age-standardized incidence rates (ASIRs), age-standardized mortality rates (ASMRs), and age-standardized DALY rates (ASDRs) per 100,000 population, with 95% uncertainty intervals (UIs) that were directly extracted from the GBD Results Tool. These UIs represent the 2.5th and 97.5th percentile values across 500 draws from the posterior distribution of each estimate, reflecting both sampling uncertainty and uncertainty arising from data source variability, model specification, and parameter estimation, as per standard GBD methodology. Temporal trends were assessed using estimated annual percentage change (EAPC) with 95% confidence intervals (CIs) [15]. The EAPC in the age-standardized rates was computed using the following formulas: y = α + βx + ε and EAPC = 100 × (exp(β) – 1), where y refers to ln (ASR), x is the calendar year, ε is the error term, and β represents the annual rate of change. These formulas are based on the linear relationship between the natural logarithm of ASR and time. The 95% CIs were determined using the linear model. The ASR trend is upward when the EAPC and the lower limit of its CI are positive; the ASR trend is downward when the EAPC and the upper limit of its CI are negative; otherwise, the ASR exhibits a stable trend. The SDI, a composite measure of development ranging from 0 to 100, was used to examine development-related disparities. SDI incorporates lag-distributed income per capita, average educational attainment among those aged 15+ years, and total fertility rate [14]. Countries were categorized into low, low-middle, middle, high-middle, and high SDI regions [16]. We used LOESS smoothing (span = 0.5) to model the nonlinear association between age-standardized rates and SDI, without applying any weighting. Spearman’s rank correlation was used to quantify the monotonic relationship. All analyses were conducted in R (version 4.3.1).
Results
Global burden of respiratory diseases in AYAs
Respiratory disease burden among AYAs varied substantially worldwide. In 2021, URIs had the highest incidence among all respiratory diseases, while TB caused the greatest mortality burden (Figure 1; Supplementary Tables SII–SXIX).
Figure 1
Global age-specific counts and proportion of incident cases and deaths by respiratory diseases type among adolescents and young adults (AYAs)
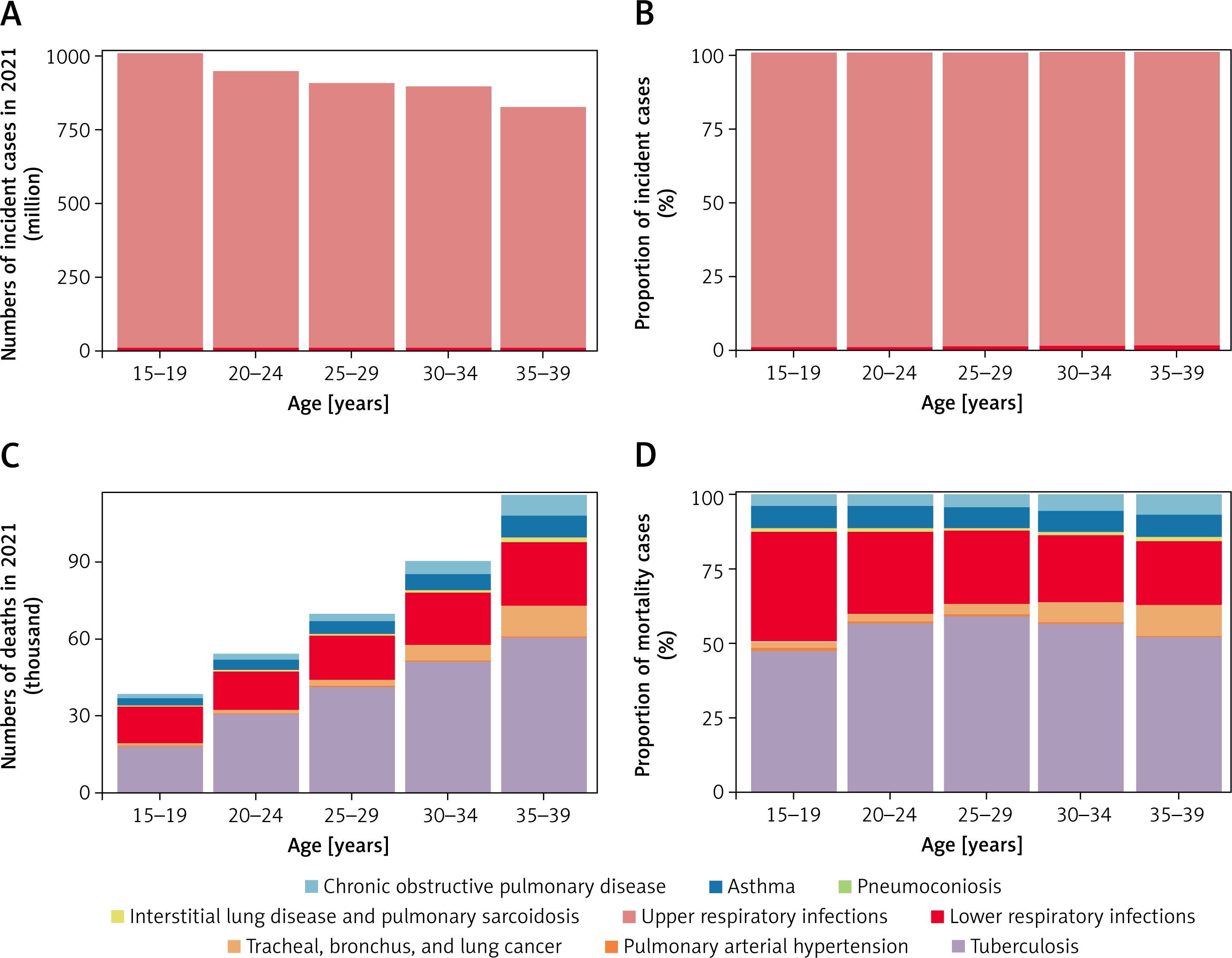
Age-specific patterns revealed contrasting trends: total incident cases declined progressively with age, whereas deaths increased. URIs and LRIs maintained consistently high incidence across all age groups. Notably, both incidence and mortality increased for COPD, pneumoconiosis, ILD/PS, TBL cancers, LRIs, and PAH, whereas asthma, URIs, and TB showed declining incidence but increasing mortality (Supplementary Table SXX).
Sex-based disparities were evident. Males had consistently higher incidence and mortality for pneumoconiosis, LRIs, and TBL cancers, whereas asthma and PAH were more prevalent in females. COPD and ILD/PS had comparable incidence between sexes but significantly higher mortality in males (Supplementary Figure S1).
Geographic distribution
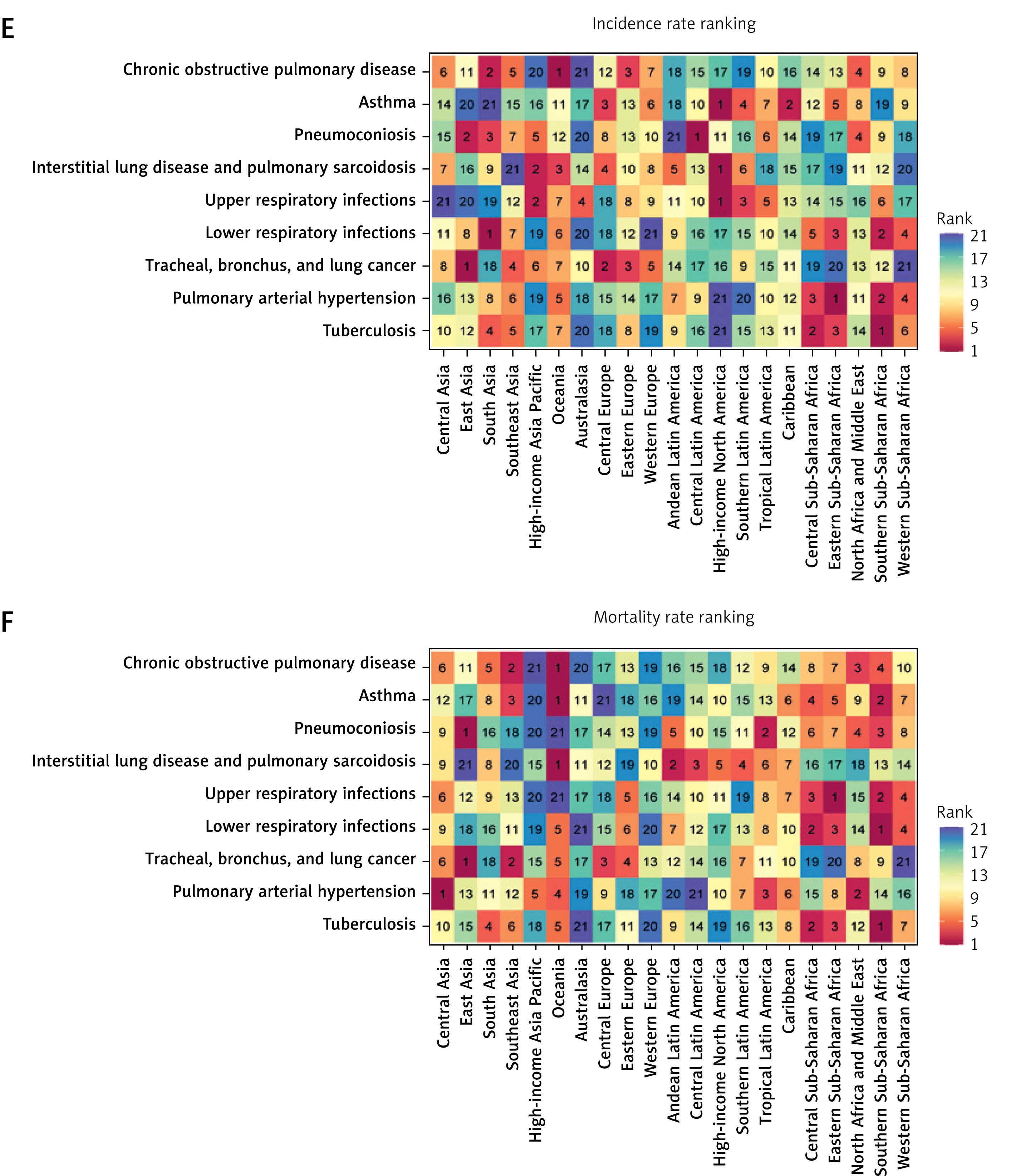
The burden of respiratory diseases showed substantial geographic variation. South Asia had the highest number of incident cases, while high-income North America led in regional ASIR and Oceania in ASMR for most disease types (Figure 2). At the national level, pneumoconiosis burden was highest in Nepal, Turkey, and Malta; PAH mortality was highest in Mongolia, Mauritius, and Tajikistan (mortality) and Zambia, Botswana, and Ethiopia (incidence). Small island nations and Southern African countries had TBL cancer and TB rankings, respectively, while high-income nations reported the highest URI incidence (Supplementary Figures S2, S3).
Figure 2
Regional burden of respiratory diseases among adolescents and young adults in 2021. Numbers of incident cases (A) and deaths (B) by region. Region-specific proportion of incident cases (C) and deaths (D) Rankings of the adolescents and young adults (AYA) respiratory diseases incidence rate (E) and mortality (F) across and within regions
Temporal trends
From 1990 to 2021, most respiratory diseases showed declining ASIRs, with TB exhibiting the most pronounced reduction (EAPC = –1.33). PAH was the only disease with an increasing ASIR (EAPC = 0.22). Similarly, ASMR decreased for most diseases, with pneumoconiosis showing the steepest decline (EAPC = –3.53), whereas ILD/PS displayed an increasing trend (EAPC = 0.61) (Supplementary Tables SII–SXIX; Supplementary Figures S4, S5). Regionally, in the Americas, LRIs were the leading cause of respiratory mortality, contrasting with TB dominance elsewhere (Supplementary Figure S6).
Correlation with SDI
Socioeconomic disparities were observed. COPD, LRIs, PAH, and TB had the highest ASIRs in low- and low-middle-SDI regions, whereas asthma, ILD/PS, and URIs predominated in high-SDI countries. Mortality patterns similarly showed disproportionately high ASMRs for asthma, URIs, LRIs, and TB in low-SDI regions (Supplementary Figure S7). An inverse association between SDI and ASIR was identified for COPD, pneumoconiosis, LRIs, PAH, and TB, while asthma, ILD/PS, URIs, and TBL cancers showed positive correlations. ASMR followed inverse patterns for most diseases, except pneumoconiosis, TBL cancer, and PAH, which correlated positively with SDI (Supplementary Figure S8).
Risk factor attribution
Risk factor analysis revealed distinct etiological patterns across diseases and sexes (Table I; Supplementary Figure S9). Air pollution was the leading global risk factor for COPD and LRIs, contributing to 32.76 DALYs for COPD and 62.37 for LRIs. Household air pollution ranked second, with both risk factors maintaining consistent rankings across sexes. Smoking was the primary COPD risk factor in high-income nations, contrasting with air pollution dominance globally.
Asthma showed sex differences: high body-mass index (BMI) was the overall leading risk factor, while occupational asthmagens predominated in males. Similarly, pneumoconiosis risk factors differed by sex: occupational carcinogens drove burden in males, whereas occupational particulate matter was principal in females. TBL cancer risk factors showed sexual dimorphism (smoking in males vs. air pollution in females), while TB burden was consistently associated with alcohol use across sexes (Table 1; Supplementary Figure S9).
Discussion
This first comprehensive analysis of respiratory disease burden among AYAs using GBD 2021 data yields four key findings. First, incidence and mortality patterns diverged markedly: URIs had the highest incidence, whereas TB had the highest mortality. Second, distinct sex disparities emerged, with male predominance in most respiratory diseases contrasting with female preponderance in asthma and PAH. Third, significant geographic disparities were evident across socioeconomic strata. Finally, we identified disease-specific risk factor profiles.
The contrasting patterns of high URI incidence and high TB mortality reflect distinct underlying mechanisms. URI transmission is unavoidable through daily social interactions [17, 18], while elevated TB mortality in AYAs stems from both immunological vulnerabilities and healthcare challenges. Adolescents exhibit immature immune responses to Mycobacterium tuberculosis, likely reflecting recent primary infection rather than reinfection immunity [19]. These biological factors combine with systemic barriers including poor treatment adherence, limited access to adolescent-friendly services, and high comorbidity burdens (HIV, diabetes, substance use, pregnancy) [20–22], underscoring the need for integrated youth-tailored interventions.
Sex disparities in respiratory diseases have important clinical implications. Males predominate in smoking-related conditions (COPD, occupational lung diseases) [23, 24], while females show greater susceptibility to asthma and PAH. The female predominance in asthma likely reflects sex-specific influences on airway physiology and immune function, with hormonal factors potentially contributing to differential susceptibility [20, 21, 25]. Similarly, PAH disproportionately affects women, with previous evidence suggesting hormonal influences on pulmonary vascular biology [26]. These findings support sex-specific management strategies, including consideration of hormonal status in asthma control and early PAH surveillance in high-risk women.
Age-related patterns reveal critical windows for intervention. COPD incidence peaked at ages 35–39 years, reflecting cumulative smoking exposure [27]. Asthma incidence was highest among adolescents but mortality peaked in middle adulthood, consistent with global patterns [28, 29]. For TB, incidence was greatest among young adults (20–24 years), with mortality peaking later (35–39 years), suggesting that progressive disease burden and treatment challenges contribute to worse outcomes with advancing age [19].
Regional variations strongly correlated with socioeconomic development. South Asia bore the heaviest burden, driven by air pollution and limited healthcare access [30]. Southern sub-Saharan Africa showed severe mortality outcomes due to diagnostic delays and inadequate treatment [31, 32], while household air pollution was a key mortality driver in Oceania [33]. Disease distribution followed clear socioeconomic gradients: COPD, LRIs, and TB clustered in lower-income regions, whereas asthma and URIs predominated in high-income areas – a pattern reflecting both true risk factor differences and surveillance biases [34, 35]. These disparities necessitate region-specific interventions: scaling up diagnostic capacity in low-resource settings, and implementing targeted asthma and URI programs in high-income areas.
Risk factor analysis revealed critical heterogeneity across populations. Air pollution was the leading risk factor for COPD among AYAs, accounting for 32.76 DALYs, suggesting particular vulnerability to environmental exposures in this age group. For asthma, high BMI was the primary risk factor (22.74 DALYs), with a stronger effect in female adolescents [36]. Socioeconomic patterns were evident: COPD in lower-income countries was mainly associated with air pollution [37, 38], whereas smoking remained dominant in high-income nations despite tobacco control policies [39]. These findings demonstrate how respiratory disease risks differ by developmental stage, sex, and environmental context, highlighting the need for tailored prevention strategies.
This study offers three key advances with practical applications: (1) identification of critical developmental windows (asthma peaking at 15–19 years, COPD emerging at 35–39 years) enables precisely timed interventions such as school-based screening and workplace prevention; (2) quantification of risk factor contributions provides evidence for context-specific resource allocation; and (3) demonstration of sex-specific patterns supports integration of hormonal considerations into clinical guidelines. These findings directly inform the World Health Organization’s Adolescent-Friendly Health Services framework [40] while highlighting the need for enhanced respiratory surveillance, particularly in under-resourced settings where diagnostic gaps may underestimate true disease burden.
Several limitations should be acknowledged. First, this study relies on modeled GBD estimates, which are contingent upon the availability and quality of primary data sources. Second, data sparsity in low- and middle-income countries may increase uncertainty, as estimates in these regions depend more heavily on predictive modeling. Third, the observed associations between disease burden and SDI are ecological in nature and should not be interpreted as causal at the individual level. Fourth, the descriptive design of this study precludes causal inference regarding the relationships between respiratory diseases and their risk factors. Additionally, residual age-related heterogeneity may persist within the broad 15–39-year range. Future studies with improved primary data collection and finer age stratification are warranted to validate our findings.
In conclusion, this study reveals that respiratory diseases pose a significant and varied burden among the AYA population globally. While URIs are most common, TB causes the most deaths. Males face higher risks from occupational exposures, while females are more vulnerable to asthma and PAH. Low-income regions struggle most with infectious and pollution-related diseases, whereas wealthier nations have more asthma cases. These findings highlight the need for tailored prevention strategies addressing specific risks by gender, age group, and region.