Current issue
Archive
Manuscripts accepted
About the Journal
Editorial office
Editorial board
Section Editors
Abstracting and indexing
Subscription
Contact
Ethical standards and procedures
Most read articles
Instructions for authors
Article Processing Charge (APC)
Regulations of paying article processing charge (APC)
UROLOGY / CLINICAL RESEARCH
Comparative analysis of prostate cancer grade at biopsy and radical prostatectomy: a retrospective observational study
1
Department of Urology and Urological Oncology, Multidisciplinary Hospital in Warsaw-Miedzylesie, Warsaw, Poland
2
Department of Urology and Andrology, Collegium Medicum, Nicolaus Copernicus University, Bydgoszcz, Poland
3
Department of Urology, Institute of Medical Sciences, Faculty of Medicine, Collegium Medicum, Cardinal Stefan Wyszyński University in Warsaw, Warsaw, Poland
4
Department of Regenerative Medicine, Collegium Medicum, Nicolaus Copernicus University, Bydgoszcz, Poland
These authors had equal contribution to this work
Submission date: 2025-11-14
Final revision date: 2026-03-17
Acceptance date: 2026-03-20
Online publication date: 2026-06-04
Corresponding author
Jędrzej J. Skorupka
Department of Urology and Urological Oncology Multidisciplinary Hospital in Warsaw-Miedzylesie Bursztynowa 2 04-749 Warsaw, Poland, Phone +48 22 47 35 149
Department of Urology and Urological Oncology Multidisciplinary Hospital in Warsaw-Miedzylesie Bursztynowa 2 04-749 Warsaw, Poland, Phone +48 22 47 35 149
KEYWORDS
TOPICS
ABSTRACT
Introduction:
Accurate Gleason grading is essential for optimal treatment selection in prostate cancer, particularly in patients eligible for active surveillance (AS). This study aimed to assess the rate of Gleason score upgrading after radical prostatectomy and its clinical implications in a large Polish cohort of patients with prostate cancer.
Material and methods:
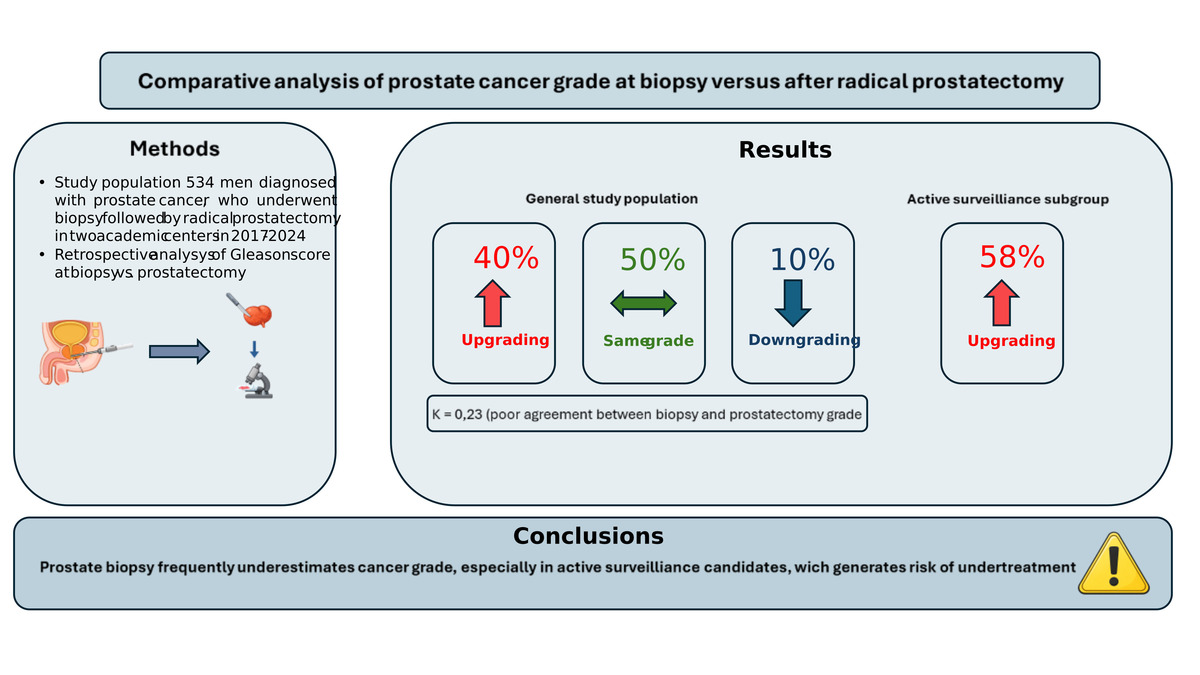
The data of 534 men with localized prostate cancer treated with radical prostatectomy at two academic centers (2017–2024) were retrospectively analyzed. Gleason scores of preoperative biopsy specimens were compared with those of whole mount prostatectomy specimens. Statistical analyses included Wilcoxon signed rank, X2, Kendall’s t, and Cohen’s k tests.
Results:
Overall, Gleason scores were upgraded in 40% of the patients, downgraded in 10%, and concordant in 50%. Among the patients meeting AS criteria at diagnosis (clinical stage ≤ T2a, PSA level < 10 ng/ml, Gleason score 3 + 3 (ISUP 1), PSA density < 0.2 ng/ml/ml, and involvement of ≤ 2 cores), upgrading occurred in 58% and downgrading in 0%. International Society of Urological Pathology grading showed a similar pattern (upgrading in 41%, downgrading in 16%). Agreement between biopsy and prostatectomy grading was low (k ≈0.23).
Conclusions:
A high Gleason upgrading rate, especially among patients who met active surveillance eligibility criteria but ultimately underwent radical prostatectomy, indicates potential underestimation of biopsy grading in routine practice. Incorporating multiparametric magnetic resonance imaging with targeted biopsy and considering centralized pathology review may improve selection for AS and reduce undertreatment of clinically significant disease. These findings underscore the limitations of biopsy-based grading in routine clinical practice and highlight the need for cautious selection of patients for active surveillance.
Accurate Gleason grading is essential for optimal treatment selection in prostate cancer, particularly in patients eligible for active surveillance (AS). This study aimed to assess the rate of Gleason score upgrading after radical prostatectomy and its clinical implications in a large Polish cohort of patients with prostate cancer.
Material and methods:
The data of 534 men with localized prostate cancer treated with radical prostatectomy at two academic centers (2017–2024) were retrospectively analyzed. Gleason scores of preoperative biopsy specimens were compared with those of whole mount prostatectomy specimens. Statistical analyses included Wilcoxon signed rank, X2, Kendall’s t, and Cohen’s k tests.
Results:
Overall, Gleason scores were upgraded in 40% of the patients, downgraded in 10%, and concordant in 50%. Among the patients meeting AS criteria at diagnosis (clinical stage ≤ T2a, PSA level < 10 ng/ml, Gleason score 3 + 3 (ISUP 1), PSA density < 0.2 ng/ml/ml, and involvement of ≤ 2 cores), upgrading occurred in 58% and downgrading in 0%. International Society of Urological Pathology grading showed a similar pattern (upgrading in 41%, downgrading in 16%). Agreement between biopsy and prostatectomy grading was low (k ≈0.23).
Conclusions:
A high Gleason upgrading rate, especially among patients who met active surveillance eligibility criteria but ultimately underwent radical prostatectomy, indicates potential underestimation of biopsy grading in routine practice. Incorporating multiparametric magnetic resonance imaging with targeted biopsy and considering centralized pathology review may improve selection for AS and reduce undertreatment of clinically significant disease. These findings underscore the limitations of biopsy-based grading in routine clinical practice and highlight the need for cautious selection of patients for active surveillance.
REFERENCES (30)
1.
Ramadani FG, Perdana NR, Ringoringo DRL. Body mass index, obesity and risk of prostate cancer: a systematic review and meta-analysis. Cent Eur J Urol 2024; 77: 176-88.
2.
Osiecki R, Kozikowski M, Białek Ł, Pyzlak M, Dobruch J. The presence of cribriform pattern in prostate biopsy and radical prostatectomy is associated with negative postoperative pathological features. Cent Eur J Urol 2024; 77: 22-9.
3.
Xu H, Zhu Y, Dai B, Ye DW. National Comprehensive Cancer Network (NCCN) risk classification in predicting biochemical recurrence after radical prostatectomy: a retrospective cohort study in Chinese prostate cancer patients. Asian J Androl 2018; 20: 551-4.
4.
Willemse PM, Davis NF, Grivas N, et al. Systematic review of active surveillance for clinically localised prostate cancer to develop recommendations regarding inclusion of intermediate-risk disease, biopsy characteristics at inclusion and monitoring, and surveillance repeat biopsy strategy. Eur Urol 2022; 81: 337-46.
5.
Carter HB, Partin AW, Walsh PC, et al. Gleason score 6 adenocarcinoma: should it be labeled as cancer? J Clin Oncol 2012; 30: 4294-6.
6.
Senkus-Konefka E, Antoniewicz A, Borkowski A, et al. Zalecenia dotyczące postępowania w raku gruczołu krokowego – konferencja okrągłego stołu. Onkol Prakt Klin 2007; 3: 103-19.
7.
Truong M, Slezak JA, Lin CP, et al. Development and multi-institutional validation of an upgrading risk tool for Gleason 6 prostate cancer. Cancer 2013; 119: 3992-4002.
8.
Altok M, Troncoso P, Achim MF, Matin SF, Gonzalez GN, Davis JW. Prostate cancer upgrading or downgrading of biopsy Gleason scores at radical prostatectomy: prediction of “regression to the mean” using routine clinical features with correlating biochemical relapse rates. Asian J Androl 2019; 21: 598-604.
9.
Smani S, Sundaresan V, Lokeshwar SD, et al. Risk factors for Gleason score upgrade from prostate biopsy to radical prostatectomy. Explor Target Antitumor Ther 2024; 5: 981-96.
10.
Allsbrook WC Jr, Mangold KA, Johnson MH, et al. Interobserver reproducibility of Gleason grading of prostatic carcinoma: general pathologist. Hum Pathol 2001; 32: 81-8.
11.
Marks L, Young S, Natarajan S. MRI-ultrasound fusion for guidance of targeted prostate biopsy. Curr Opin Urol 2013; 23: 43-50.
12.
Huang TH, Li WM, Ke HL, et al. The factors impacting on Gleason score upgrading in prostate cancer with initial low Gleason scores. J Formos Med Assoc 2025; 124: 145-50.
13.
Ozkan TA, Eruyar AT, Cebeci OO, Memik O, Ozcan L, Kuskonmaz I. Interobserver variability in Gleason histological grading of prostate cancer. Scand J Urol 2016; 50: 420-4.
14.
Khoddami M, Khademi Y, Kazemi Aghdam M, Soltanghoraee H. Correlation between Gleason scores in needle biopsy and corresponding radical prostatectomy specimens: a twelve-year review. Iran J Pathol 2016; 11: 120-6.
15.
Boccon-Gibod L, Bertaccini A, Bono AV, et al. Management of localized prostate cancer by radical prostatectomy in Europe in 2005. Eur Urol 2005; 48: 580-4.
16.
Duffield AS, Lee TK, Miyamoto H, Carter HB, Epstein JI. Radical prostatectomy findings in patients in whom active surveillance of prostate cancer fails. J Urol 2009; 182: 2274-8.
17.
Epstein JI, Feng Z, Trock BJ, Pierorazio PM. Upgrading and downgrading of prostate cancer from biopsy to radical prostatectomy: incidence and predictive factors using the modified Gleason grading system and factoring in tertiary grades. Eur Urol 2012; 61: 1019-24.
18.
Schoots IG, Petrides N, Giganti F, et al. Magnetic resonance imaging in active surveillance of prostate cancer: a systematic review. Eur Urol 2015; 67: 627-36.
19.
Shill DK, Roobol MJ, Ehdaie B, Vickers AJ, Carlsson SV. Active surveillance for prostate cancer. Transl Androl Urol 2021; 10: 2809-19.
20.
Bott SRJ, Young MP, Kellett MJ, Parkinson MC; Contributors to the UCL Hospitals’ Trust Radical Prostatectomy Database. Anterior prostate cancer: is it more difficult to diagnose? BJU Int 2002; 89: 886-9.
21.
Fine SW, Epstein JI. A contemporary study correlating prostate needle biopsy and radical prostatectomy Gleason score. J Urol 2008; 179: 1335-8; discussion 1338.
22.
Ankerst DP, Xia J, Thompson IM Jr, et al. Precision medicine in active surveillance for prostate cancer: development of the canary-early detection research network active surveillance biopsy risk calculator. Eur Urol 2015; 68: 1083-8.
23.
Diniz CP, Landis P, Carter HB, Epstein JI, Mamawala M. Comparison of biochemical recurrence-free survival after radical prostatectomy triggered by grade reclassification during active surveillance and in men newly diagnosed with similar grade disease. J Urol 2017; 198: 608-13.
24.
Tosoian JJ, Mamawala M, Epstein JI, et al. Active surveillance of Grade Group 1 prostate cancer: long-term outcomes from a large prospective cohort. Eur Urol 2020; 77: 675-82.
25.
Choudhary MK, Kolanukuduru KP, Tillu N, et al. Lesion volume on multiparametric magnetic resonance imaging as a non-invasive prognosticator for clinically significant prostate cancer. Cent Eur J Urol 2024; 77: 592-8.
26.
Rempega G, Rajwa P, Ryszawy J, et al. The influence of the operator’s experience on the outcomes of fusion prostate biopsy. Cent Eur J Urol 2023; 76: 287-92.
27.
Hamdy FC, Donovan JL, Lane JA, et al. 10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N Engl J Med 2016; 375: 1415-24.
28.
de Reijke TM, van Moorselaar JR. Re: ten-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. Eur Urol 2017; 71: 491-2.
29.
Cooperberg MR. Re: 10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. Eur Urol 2017; 71: 492-3.
30.
Albertsen PC. Re: 10-year outcomes after monitoring, surgery or radiotherapy for localized prostate cancer. Eur Urol 2017; 72: 470.
Share
RELATED ARTICLE
| eISSN: | 1896-9151 |
| ISSN: | 1734-1922 |
We process personal data collected when visiting the website. The function of obtaining information about users and their behavior is carried out by voluntarily entered information in forms and saving cookies in end devices. Data, including cookies, are used to provide services, improve the user experience and to analyze the traffic in accordance with the Privacy policy. Data are also collected and processed by Google Analytics tool (more).
You can change cookies settings in your browser. Restricted use of cookies in the browser configuration may affect some functionalities of the website.
You can change cookies settings in your browser. Restricted use of cookies in the browser configuration may affect some functionalities of the website.