Introduction
In children, recurrent pain in the feet and/or lower limbs is a major cause of concern for many parents and among the most frequent reasons for consultation in pediatric healthcare.
Lower limb pain is a clinical entity for which an unambiguous cause has yet to be established, although many proposals have been made, including fatigue theory, anatomical theory, emotional theory and growth theory. The problem is particularly acute among children aged 3–12 years, with a reported prevalence ranging from 2.6% to 49.4% [1].
Childhood and juvenile obesity is a multifactorial disease characterized by the excessive accumulation of fat mass. It is a major health problem worldwide, and in the medium-long term, its consequences may provoke a public health crisis [2].
The prevalence of overweight and obesity varies widely, from 7% to 40%, according to geographical area and the measurement criteria used. However, the prevalence of childhood obesity in Spain is undoubtedly among the highest in Europe [3–5].
The direct consequences of childhood obesity are very worrying, given its relationship with obesity in adulthood [6] and its association with significant increases in comorbidity and disability [7].
Childhood obesity affects the functional characteristics of the lower limb, and can predispose children to pain and discomfort while walking, as well as musculoskeletal comorbidities [8], reduced hip and knee flexion during walking and increased valgus knee deformity [9]. Relative to osteoarticular problems low back pain is the most frequent symptom [10].
These research findings support the view that obesity predisposes to joint dysfunction and corroborate a theoretical association with musculoskeletal pathology. Nevertheless, few studies have been undertaken to document the impact of childhood obesity on the feet and lower limbs.
The distal location and flexibility of the pediatric foot make it especially susceptible to pathology and deformation. Accordingly, any external influence on the developing foot, such as obesity, may affect its function during walking [11].
In addition, plantar pressure and arch height can be affected as a consequence of obesity alterations in children [12, 13].
The main aim of this study, therefore, is to describe the relationship between childhood overweight and obesity and foot/lower limb pain in a population of primary school children in Spain.
Material and methods
Study design and participants
The cross-sectional descriptive study analyzed a population of 150 children aged 9 to 12 years attending a primary school in Malaga (southern Spain), following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) [14]. None had pathologic feet.
The required sample size was estimated using two series model correlation tests using the G*Power 3.1.9.2 software (G*Power; Dusseldorf University; Germany). In addition, a moderate correlation coefficient of r = 0.4 [15], a two-tailed hypothesis, an error of α = 0.05, and a power of error probability of 1 – β = 0.80 were considered. Thus, a sample size of 144 subjects was considered to achieve an actual power of 0.807.
The inclusion criteria were: symmetry in the feet, no joint deformities, age 9–12 years and written informed consent provided by parents or guardians.
The exclusion criteria were: presence of joint or bone disease, history of surgery in the lower limbs, morphologic alterations in the feet, lower limb injuries that caused pain, neurological abnormalities in the lower limb, alterations in the skin of the feet or plantar verruca.
Study variables
The dependent variables were pain in the feet and/or the lower limbs, i.e. the thigh (the upper leg: femur), the leg (the lower leg: tibia, fibula and patella) and/or the foot.
The predictor variables were: age, sex, body mass index (BMI), sport activity, foot posture index (FPI) and knee alignment.
Measurement of the variables
Also obtained during the physical examination were the foot posture index (FPI) [16] and the angular deviations (or alignment) of the knees (genu varum and genu valgum) [17].
To obtain these measurements, the participants were instructed to remain in a standing position for approximately 2 min with their arms relaxed by their side, and looking straight ahead. In the present study, taking into account that the FPI has proven good intra-observer reliability but only moderate interobserver reliability, the same examiner took all the measurements.
For this purpose, the following parameters were considered: palpation of the astragalus head, inframalleolar and supramalleolar curvature, the position of the calcaneus in the frontal plane, the prominence of the astragalus-scaphoid articulation, and the abduction-adduction of the forefoot. The possible scores awarded for each criterion were –2, –1, 0, 1, or 2.
Knee alignment was measured as the intermalleolar or intercondylar distance, using a graduated ruler. The children were measured in an orthostatic position, observed in the posteroanterior direction, as recommended in the literature [18]. An intermalleolar distance of 8 cm or more was considered indicative of valgus knee, and an intercondylar distance of 6 cm or more was indicative of varus knee, for all ages. The latter distance was measured with the medial malleoli in contact and was less than 6 cm in the children with genu varum. The intermalleolar distance was measured with the knees in contact, and was less than 8 cm in the children with genu valgum [19].
Data collection
Each participant was examined by two researchers, working independently and following a pre-established procedure (examination guide). When any type of alteration or pathology was detected or suspected, the parents or guardians were given a consultation request form and recommended to visit a podiatric physician, pediatrician or orthopedist to confirm the diagnosis and administer the appropriate treatment.
Statistical analysis
To preserve data independence, and in view of the strong correlation observed in previous studies between FPI scores for left and right feet [20], although both were measured, for further statistical analysis only one foot (the left, chosen at random) was included in the statistical analysis.
A descriptive analysis was performed of the quantitative variables, obtaining measures of central tendency and dispersion, and of the qualitative ones with frequencies and percentages. Association analysis was performed using the χ2 test, with Fisher’s adjustment if necessary, and by calculating the unadjusted odds ratio (UOR) and the corresponding 95% confidence intervals.
Finally, a multivariate analysis was conducted, using binary logistic regression, seeking to identify factors related to the dependent variables (foot and lower limb pain) and to control for potential confounding variables. The predictive variables included in the binary logistic regression model were age, sex, sport activity, knee alignment, FPI and BMI. In addition, the adjusted odds ratios (AOR) and the corresponding 95% CI were calculated.
All statistical information was analyzed using SPSS software (IBM SPSS Statistics for Windows, version 23.0, IBM Corp., Armonk, NY, licensed to the Central Computer System of the University of Malaga, Spain). A p-value < 0.05 was considered statistically significant.
Ethical considerations
This study was approved by the Ethics and Research Committees of the University of Malaga, which confirmed that the study was performed in accordance with all ethical standards and the relevant provisions of the Declaration of Helsinki [21].
In addition, the study was approved by the principal of the primary school concerned. In every case, the parents or guardians provided written informed consent for their children to participate in this study. They were also asked to complete a survey about podiatric medical habits. Data confidentiality was maintained at all times in accordance with current legislation in this respect, i.e. EU Regulation 2016/679 of the European Parliament and of the Council, of 27 April 2016, on the protection of natural persons with regard to the processing of personal data and the free movement of such data.
Results
Interviews were conducted with 150 children who met the eligibility criteria. Their mean age was 10.21 ±1.00 years; 47.3% were girls, 15.3% were overweight and 12.7% were obese. The overall prevalence of foot pain was 10.7% and that of lower limb pain, 27.3%.
Table I Details the characteristics of the participants, in total and by sex. Of the 150 children, none presented FPI values corresponding to highly supinated, supinated or highly pronated feet. Thus, 76 (50.7%) were classed as neutral and 74 (49.3%) were pronated. A slightly higher proportion of the girls had pronated feet (52.1%) and genu valgum (45.1%). The respective values for the boys were 46.8% and 21.1%. As concerns sport activity, 89.9% of the boys and 83% of the girls were active in this respect.
Table I
Characteristics of the total sample and by sex
Table II shows the prevalence of foot/lower limb pain recorded, according to each of the study variables. No significant differences were observed in relation to age and sex. The only study variable that was significantly related to both foot pain and lower limb pain was overweight/obesity (UOR = 4.05; 95% CI: 1.24–13.22; p = 0.014 and UOR = 3.57; 95% CI: 1.66–7.66; p = 0.001 respectively). Likewise, the study subjects with a pronated foot had a significantly higher prevalence of lower limb pain than those whose FPI was within normal parameters (UOR = 2.54; 95% CI: 1.20–5.38; p = 0.013).
Table II
Prevalence of foot/lower limb pain depending on the study variables (N = 150)
| Variables | Categories | Foot pain | Lower limb pain | ||||
|---|---|---|---|---|---|---|---|
| Pain (%) | UOR (CI) | P-value | Pain (%) | UOR (CI) | P-value | ||
| Age | 9–10 | 12.0 | 1 | 0.708 | 28.3 | 1 | 0.891 |
| 11–12 | 8.6 | 0.90 (0.53–1.53) | 25.9 | 0.97 (0.68–1.40) | |||
| Sex | Male | 13.9 | 1 | 0.173 | 29.1 | 1 | 0.606 |
| Female | 7.0 | 0.47 (0.15–1.42) | 25.4 | 0.83 (0.40–1.70) | |||
| Sport activity | No | 10.0 | 1 | 0.917 | 30.0 | 1 | 0.774 |
| Yes | 10.8 | 1.09 (0.23–5.18) | 26.9 | 0.86 (0.31–2.41) | |||
| Knee alignment | Neutral | 10.6 | 1 | 0.964 | 25.5 | 1 | 0.484 |
| Genu varum | 0.0 | 0.00 | 14.3 | 0.49 (0.06–4.24) | |||
| Genu valgum | 12.2 | 1.17 (0.40–3.44) | 32.7 | 1.41 (0.66–3.01) | |||
| FPI | Neutral | 6.6 | 1 | 0.100 | 18.4 | 1 | 0.013* |
| Pronated | 14.9 | 2.48 (0.82–7.52) | 36.5 | 2.54 (1.20–5.38) | |||
| BMI | Normal | 4.9 | 1 | 0.014* | 16.0 | 1 | 0.001* |
| Overweight/obesity | 17.4 | 4.05 (1.24–13.22) | 40.6 | 3.57 (1.66–7.66) | |||
In addition, a statistically significant relationship was observed between overweight/obesity and genu valgum (UOR = 4.93; 95% CI: 2.34–10.37; p < 0.001).
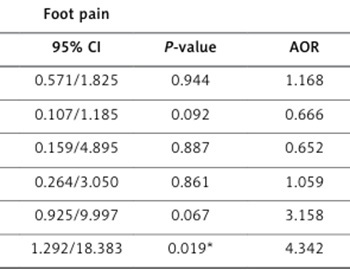
Finally, a multivariate logistic regression was conducted to identify independent factors for foot/lower limb pain. The adjusted ORs (AORs) and 95% CIs obtained by multivariable logistic regression for foot/lower limb pain are shown in Table III. The multivariate analysis identified children with overweight or obesity as being more likely to experience foot/lower limb pain than those with normal weight (AOR = 4.874; 95% CI: 1.292–18.383; p = 0.019 and AOR = 4.342; 95% CI: 1.792–10.521; p = 0.001 respectively). In addition, a statistically significant relationship was observed between pronated foot and lower limb pain (AOR = 3.158; 95% CI: 1.390–7.176; p = 0.006).
Table III
Study variables related to foot/lower limb pain (logistic regression)
| Variables | Foot pain | Lower limb pain | ||||
|---|---|---|---|---|---|---|
| AOR | 95% CI | P-value | AOR | 95% CI | P-value | |
| Agea | 1.021 | 0.571/1.825 | 0.944 | 1.168 | 0.771/1.769 | 0.463 |
| Sexb | 0.356 | 0.107/1.185 | 0.092 | 0.666 | 0.293/1.512 | 0.331 |
| Sport activityc | 0.883 | 0.159/4.895 | 0.887 | 0.652 | 0.205/2.074 | 0.469 |
| Knee alignmentd | 0.897 | 0.264/3.050 | 0.861 | 1.059 | 0.435/2.581 | 0.899 |
| FPIe | 3.041 | 0.925/9.997 | 0.067 | 3.158 | 1.390/7.176 | 0.006* |
| BMIf | 4.874 | 1.292/18.383 | 0.019* | 4.342 | 1.792/10.521 | 0.001* |
Discussion
The results obtained in the present study indicate a high prevalence of foot and lower limb pain in children aged 9–12 years with overweight or obesity. Specifically, these children had a higher prevalence of pain in the feet (17.4% vs. 4.9%; p = 0.014) and in the lower limbs (40.6% vs. 16%; p = 0.001) compared to children with normal weight.
A previous study in this field [22] identified a relationship between musculoskeletal pain in the lower limbs and overweight and childhood obesity, and emphasized the negative impact produced by elevated BMI on the general health and psychosocial well-being of the child. Similarly, Bout-Tabaku et al. [23] observed that obese children had poorer psychosocial health than their contemporaries with normal weight, as well as a generally worse physical condition.
Butterworth et al. [24] reviewed several studies of the association between BMI and musculoskeletal foot disorders, and concluded that there was a strong association between increased BMI, chronic heel pain and nonspecific foot pain. In another study, Yan et al. [25] observed that obese children had weaker walking stability, a flatter foot pattern, a larger foot axis angle and an altered distribution of dynamic plantar pressures, compared to non-obese children.
The results of the present study show that 27.3% of the children presented pain in one or more locations in the lower limbs, while 10.7% only had pain in the feet. Brady et al. [26] observed that that obesity was a risk factor for musculoskeletal pain in multiple sites of the lower limbs, and that this multiplicity was more frequent than pain in a single location.
We also detected a significant relationship between overweight-obesity and genu valgum, thus corroborating prior research by Maciałczyk-Paprocka et al. [27] and Gonçalves de Castro et al. [28], who established a relationship between obesity and overweight (measured by BMI) and incorrect body posture in children and adolescents. Both of these studies concluded that overweight and obesity in children and adolescents predispose to a higher incidence of postural alterations such as valgus knees and pronounced feet.
Our analysis also highlighted the existence of a statistically significant relationship between pain in the lower limbs and a pronated FPI, although no such relationship was found between the FPI and the BMI. In this respect, Mahaffey et al. [29] indicated the existence of a more pronated type of foot in children with greater body fat and with a predisposition to pain and discomfort during weight-bearing activities, suggesting that the latter circumstance would reduce the children’s motivation to carry out physical activities.
On the other hand, Gonçalves de Carvalho et al. [30] found that persons with pronated feet had a BMI within the normal range. Similarly, Gijon-Nogueron et al. [10] observed no statistically significant relationship between elevated BMI and the existence of pronated foot.
From another perspective, Walsh et al. [31] studied the relationship between foot pain and obesity in adults, reporting that as body weight increases, so does plantar pressure, thereby increasing pain in the foot. Further research should be undertaken to corroborate these findings, with a study population of children. It may be hypothesized that when the foot must bear greater weight, pressure and load on a relatively small plantar surface, it will be subjected to greater reaction forces when walking, triggering pain in the feet and lower limbs. Moreover, skeletal deformities may be provoked by the pressure resulting from weight gain. Further studies of issues related to childhood obesity and foot pain, based on a longitudinal and analytical design, are necessary.
In addition, health-related quality of life or even in another chronic diseases as the case of arthritis rheumatoid, risk of fall or infection can be affected by obesity in the general population or children [32–34].
Podiatrists should consider the effect of increased body weight on plantar load in overweight and obese children. When weight loss, through diet and/or exercise, reduces the mass of adipose tissue, this may lessen the risk of pain in the lower limbs and in the foot. Consequently, weight loss and lifestyle changes should be considered in the case of children presenting overweight or obesity, in order to forestall or alleviate lower limb pain and foot pain in adulthood, as well as relative aspect related to the promotion of podiatric health [35].
The present study is subject to certain limitations. The first is that of its cross-sectional design, which precludes the establishment of direct causal relationships. However, the identification of factors related to foot and lower limb pain, which was one of the main study aims, is well within the capabilities of this type of study. Another limitation is the high interobserver variability intrinsic to the FPI. In order to minimize the effects of this problem, each participant was examined individually by two researchers, following a pre-established examination procedure (examination guide).
In conclusion, overweight and obesity are the main factors related to pain in the feet and lower limbs in primary school children. Children with pronated feet have a greater prevalence of lower limb pain than children whose FPI parameters are within the range of normal values. Overweight and obesity are also risk factors for genu valgum.