Introduction
Pancreatic cancer (PC), which is associated with an unfavourable prognosis, is the fourth most common cause of death worldwide [1, 2]. In 2018, 432,242 PC-related deaths were reported, accounting for 4.5% of all deaths caused by cancer, and placing it 11th among the world’s most common cancers, according to the report published by GLOBOCAN 2018 [3]. Surgical resection is the only potentially curative option for patients with PC. Only a minority of PC patients are presented at a curatively resectable stage at the initial diagnosis [4]. The five-year survival rate in PC remains at only < 5% despite decades of efforts in surgical and medical treatment [5]. Although several clinical prognostic factors related to PC have been explored, they still fail to accurately predict the outcome of individual patients. Thus, it is of great significance to explore novel biomarkers to predict prognosis and provide timely and effective therapeutic strategies for PC patients.
E-cadherin (CDH1) is a calcium-dependent transmembrane glycoprotein that mediates cell-cell adhesion between epithelial cells. CDH1 also plays a crucial role in the metastasis and invasion of different types of cancer [6–8]. The downregulation or loss of CDH1 expression may cause some changes related to pathology, tumour cell dedifferentiation, and uncontrolled growth [9, 10]. To date, correlation between CDH1 expression and the prognosis of PC patients has attracted the attention of scholars. However, controversial results have been reported. Fei et al. [11] recruited 58 patients with PC, including 37 males and 11 females, and found that loss of CDH1 protein expression was associated with a worse prognosis, while normal expression of CDH1 had a superior survival rate for PC patients. Radulovic et al. [12] obtained 61 tumour pancreatic tissue samples from patients (30 males and 31 females, range of age: 32–78 years) with pancreatic ductal adenocarcinoma (PDAC), who underwent pancreatectomy. They inferred that low expression of CDH1 had a negative impact on patient survival. However, Grupp et al. [13] collected 34 specimens of PC and presented controversial results. They reported that the expression of CDH1 was not markedly associated with metastatic disease, and CDH1, as a prognostic marker, was excluded in the study of patients with PDAC.
However, the above-mentioned studies suffered from a lack of comprehensive support from evidence-based medicine, as well as the existence of considerable controversy. Therefore, the purpose of this study was to assess the prognostic value of CDH1 in PC patients by performing a meta-analysis.
Material and methods
Search method
The present meta-analysis was conducted according to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-P) [14].
We searched for relevant articles published up to September 2018 via the PubMed and Embase databases. The searched terms were: “E-cadherin or cadherin 1 or CDH1 or E-cad or Epithelial cadherin” and “pancreatic cancer or pancreatic carcinoma or PDAC or pancreatic tumor or pancreatic malignant or pancreatic ductal adenocarcinoma or pancreatic neoplasms” and “outcome or survival or prognoses or prognostic or prognosis”. Furthermore, we manually searched for all relevant articles.
Inclusion and exclusion criteria
Inclusion criteria were as follows: (1) Patients with PC confirmed by histopathological examinations; (2) the full text of article was published in English; (3) hazard ratios (HRs) and 95% confidence intervals (95% CIs) were directly calculated from data reported; (4) the expression of CDH1 was detected in human primary tumour tissues; and (5) immunohistochemistry (IHC) was applied to measure the expression level of CDH1 in the primary PC tissues.
We excluded publications with the following criteria: (1) duplicate publications; (2) editorials, conference abstracts, letters, or reviews.
Data extraction
The following data were collected: the first author’s full-name, country, ethnicity, year of publication, number of patients, age, tumour grade, TNM stage, lymph node metastasis, invasion depth, tumour differentiation, distant metastasis and vascular invasion, as well as HR and 95% CI for CDH1 expression-related overall survival (OS). The multivariate values were preferentially chosen whenever the study provided both multivariate and univariate HRs. If HR and 95% CI were not given directly, these values were calculated using the Kaplan-Meier (K-M) curve via Engauge Digitizer version 4.1 to extract the survival rates and HR according to the method of Tierney et al. [15, 16]. These data were extracted by two reviewers independently. Discrepancies in our results were resolved by discussion.
Assessment of quality
The Newcastle-Ottawa scale (NOS) was used to assess the quality of nonrandomised studies. Two investigators independently assessed the quality of 16 studies. In the NOS system [17], low-quality studies achieving NOS scores of < 6 were excluded. High-quality studies, which were included in the current meta-analysis, attained NOS scores of ≥ 6.
Statistical analysis
STATA 12.0 software (StataCorp, College Station, TX, USA) was adopted to perform all the statistical analyses in the present meta-analysis. c2-based Q test and I2 index were used to assess heterogeneity among the included studies. P < 0.10 and I2 > 50% indicated that there was a substantial heterogeneity, and the random-effects model was utilised to carry out pooled analysis of data. Otherwise, the fixed-effect model was chosen. A combined HR > 1 indicated an unfavourable prognosis for PC patients with reduced expression of CDH1. If 95% CIs for overall HR were not greater than 1.0, the prognostic effect of CDH1 was statistically significant. In order to study correlation between clinicopathological features and CDH1 expression, odds ratio (OR) with 95% CI was used. If 95% CI and OR were no greater than 1.0, the decrease of CDH1 expression was statistically significant with clinical features. Subsequently, we performed subgroup analysis to explore the association between CDH1 expression and OS. The sensitivity analysis was conducted to test the stability of studies on the final effect by sequentially omitting individual studies. The Egger’s and Begg’s tests were used to assess publication bias, and p < 0.05 was deemed to prove publication bias. Begg funnel plots were employed to visually investigate potential publication bias, in which a symmetric plot suggested no publication bias.
Results
Selection of eligible studies
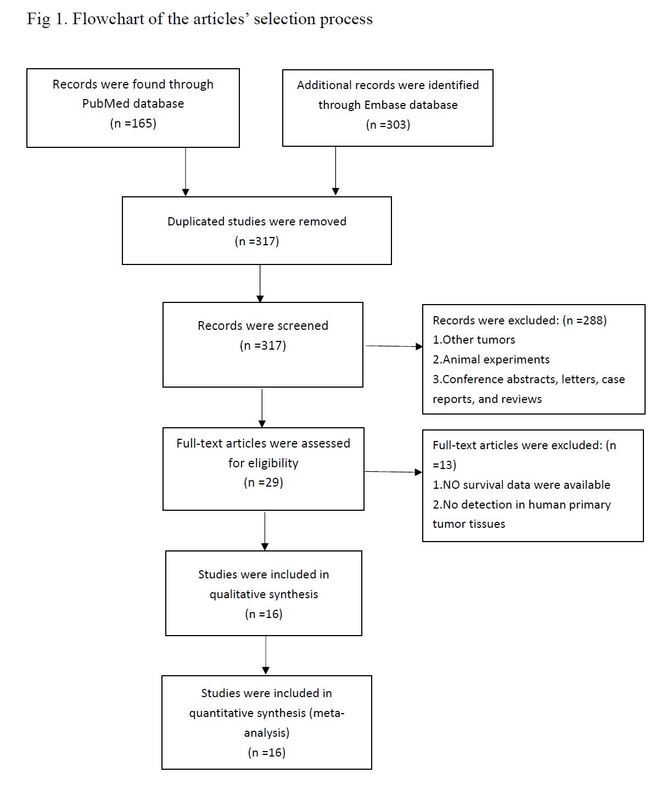
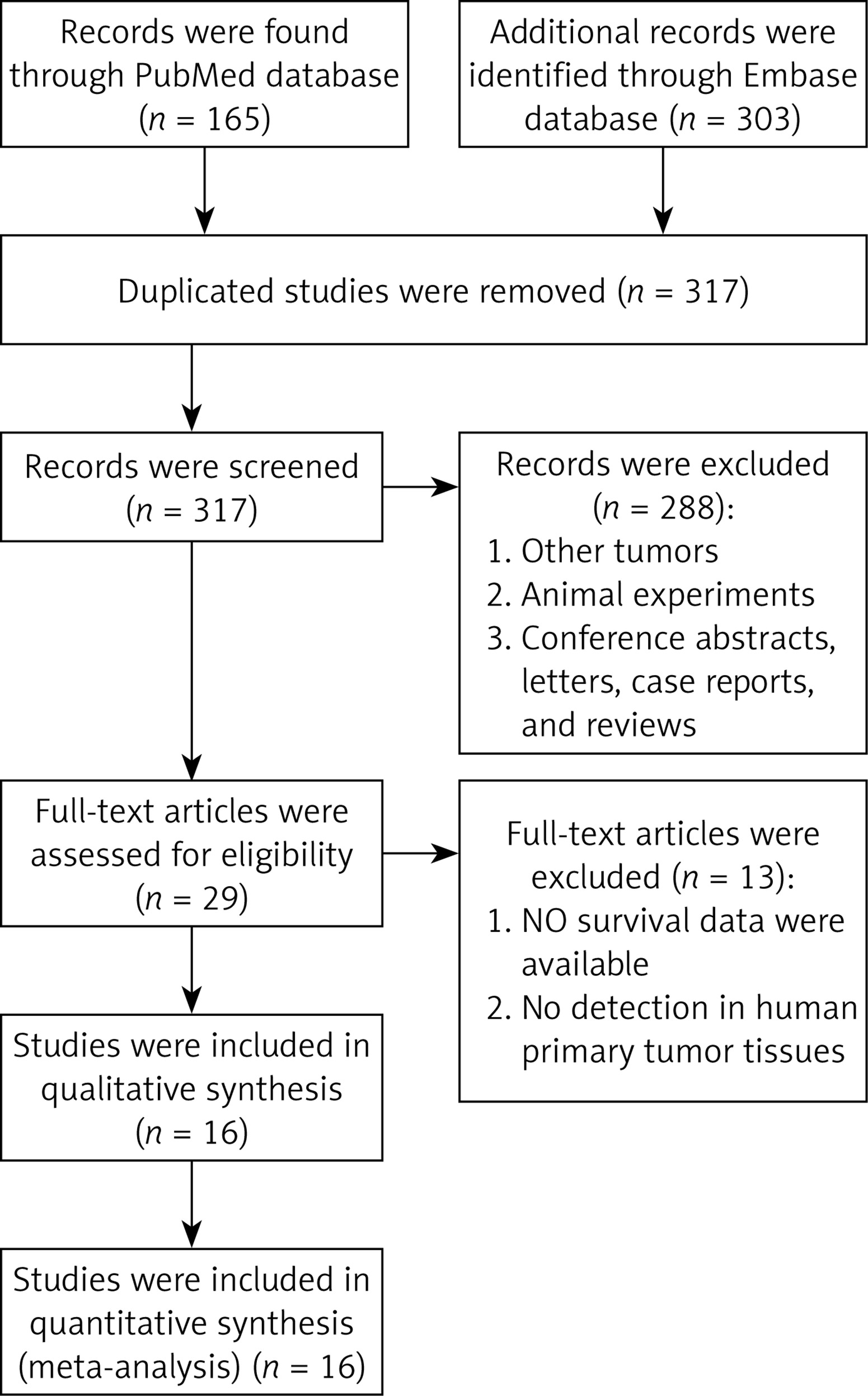
As shown in Figure 1, 468 citations (Pubmed (n = 165), Embase (n = 303)) were identified using the described search strategies. In total, 151 duplicated studies were removed and 317 remained. Subsequently, a further 288 articles were excluded through screening titles and abstracts for the following reasons: conference records, abstracts, reviews, comments, and experimental studies. Then we systematically reviewed the full text of the remaining 29 articles and screened out another 13 articles due to the insufficient survival data. In total, 16 articles [11, 12, 18–31] were involved in the present meta-analysis.
Characteristics of included studies
The primary features of all included articles are shown in Table I. The 16 published studies between 2003 and 2018 included a total of 1805 patients. The number of samples involved in each study ranged from 34 to 329 with a mean age of 58–67 years. The CDH1 reactivity was detected in all eligible studies using immuno-histochemistry (IHC). Reduced E-cadherin expression was defined by the use of different cut-off values among different studies; therefore, we classified all patients according to the original studies (reduced or normal staining).
Table I
Characteristics of included studies
| First author | Year | Country | Ethnicity | No. of patients | Survival | Methods | Cut-off value | Pathologist | HR estimated | OS HR (95% CI) | Mean age [year] | NOS | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Selection | Comparability | Outcome | ||||||||||||
| Shimamura [30] | 2003 | Japan | Asian | 125 | OS | IHC | 90% | Na | Given by author | 1.82 (1.17–2.83) | 63.1 | ★★★☆ | ★★ | ★★★ |
| Shin [31] | 2005 | South Korea | Asian | 53 | OS | IHC | 70% | Yb | Survival curves | 1.18 (0.63–2.22) | 58 | ★★★☆ | ★★ | ★★☆ |
| Oida [29] | 2006 | Japan | Asian | 72 | OS | IHC | NA | N | Survival curves | 1.61 (0.98–2.63) | 63.2 | ★★★☆ | ★★ | ★★☆ |
| Javle [28] | 2007 | USA | Caucasian | 34 | OS | IHC | SSS score < 100 | Y | Survival curves | 1.83 (0.45–7.35) | 66 | ★★★☆ | ★★ | ★★☆ |
| Fei [11] | 2010 | China | Asian | 58 | OS | IHC | 90% | Y | Survival curves | 2.04 (1.11–3.70) | NR | ★★★☆ | ★★ | ★★☆ |
| Karamitopoulou [27] | 2010 | Switzerland | Caucasian | 196 | OS | IHC | NA | Y | Survival curves | 1.49 (1.05–2.13) | 66.5 | ☆★★☆ | ★★ | ★★★ |
| Hong [26] | 2011 | USA | Caucasian | 329 | OS | IHC | 5% | N | Survival curves | 1.43 (1.15–1.76) | 66.5 | ★★★☆ | ★★ | ★★★ |
| Handra-Luca [25] | 2014 | France | Caucasian | 99 | OS | IHC | NA | N | Given by author | 4.18 (1.81–9.68) | NR | ☆★★☆ | ★★ | ★★☆ |
| Yamazaki [24] | 2014 | Japan | Asian | 113 | OS | IHC | NA | N | Given by author | 0.88 (0.48–1.61) | 65 | ☆★★☆ | ★★ | ★★☆ |
| Kohler [23] | 2015 | Germany | Caucasian | 103 | OS | IHC | 50% | Y | Survival curves | 1.21 (0.48–3.06) | 67 | ★★★☆ | ★★ | ★★★ |
| Chen [22] | 2016 | China | Asian | 90 | OS | IHC | IHC score ≤ 1 | Y | Given by author | 1.59 (0.47–3.45) | 62 | ★★★☆ | ★★ | ★★★ |
| Han [21] | 2016 | China | Asian | 84 | OS | IHC | IHC score ≤ 4 | N | Given by author | 2.09 (1.20–3.61) | 62 | ☆★★☆ | ★★ | ★★★ |
| Chen [20] | 2017 | China | Asian | 80 | OS | IHC | IHC score ≤ 4 | N | Given by author | 1.73 (1.00–2.99) | NR | ☆★★☆ | ★★ | ★★☆ |
| Kawanishi [19] | 2017 | Japan | Asian | 256 | 0S | IHC | 30% | N | Given by author | 0.89 (0.67–1.19) | 66.8 | ★★★☆ | ★★ | ★★★ |
| Wang [18] | 2018 | China | Asian | 52 | 0S | IHC | IHC score < 4 | Y | Survival curves | 1.69 (0.82–3.47) | 65.6 | ★★★☆ | ★★ | ★★☆ |
| Radulovic [12] | 2018 | Croatia | Asian | 61 | OS | IHC | 5% | N | Survival curves | 1.42 (0.66–3.04) | 62 | ★★★☆ | ★★ | ★★★ |
HR – hazard ratio, OS – overall survival, CI – confidence interval, IHC – immunohistochemistry, NOS – Newcastle-Ottawa scale, NA – not available, SSS – semiquantitative scoring system, IHC score – staining intensity × staining distribution, SSS score – staining intensity + the percentage of stained cells,
Quality assessment
Based on NOS scores, three parameters were evaluated in terms of the following: selection, comparability, and outcomes. All the involved studies were of high quality, with scores ≥ 6 (Table I).
The relationship between CDH1 expression and prognosis in PC patients
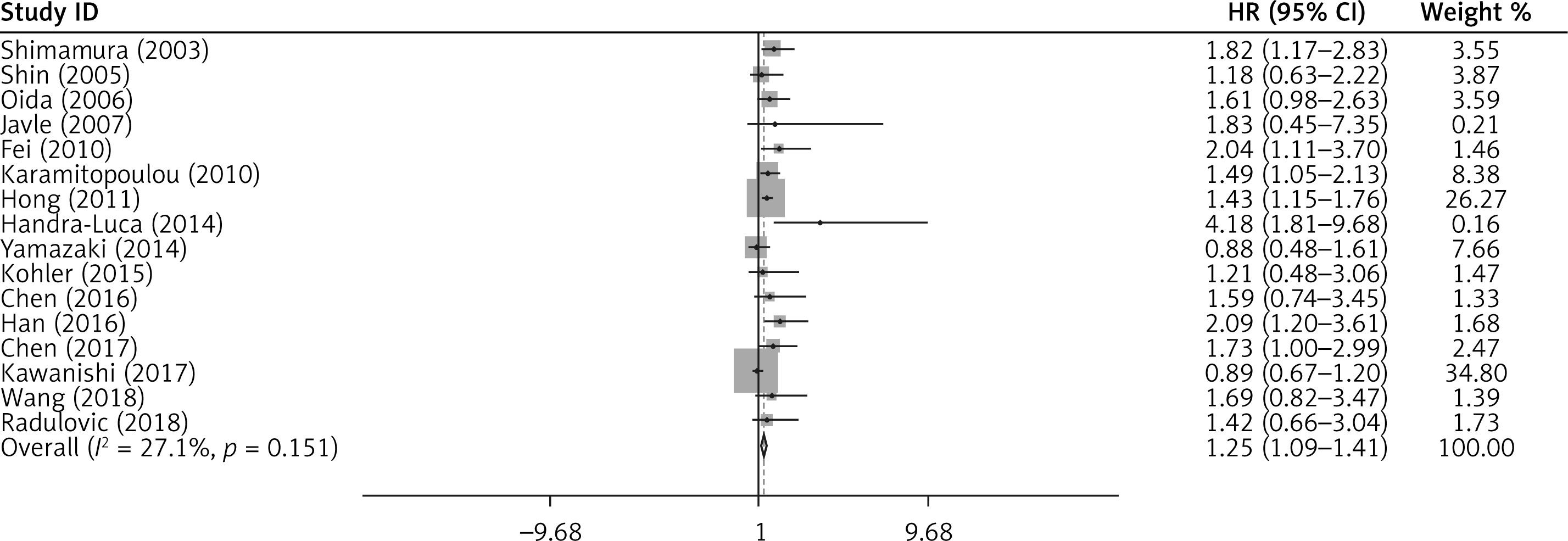
According to the results of the 16 included studies, a forest plot of the individual HR was drawn, and the results of the present meta-analysis are shown in Figure 2. It was revealed that CDH1 expression was negatively correlated with adverse OS (pooled HR = 1.25, 95% CI: 1.09–1.41, p < 0.001). The fixed-effects model was chosen due to the low heterogeneity (I2 = 27.1%, p = 0.151).
Figure 2
Forest plot of hazard ratio (HR) for the correlation between reduced expression of CDH1 and overall survival in pancreatic cancer patients
Subgroup analyses were performed to investigate the association between reduced expression of CDH1 and OS on the basis of ethnicity, year of publication, study country, patients’ mean age, and survival analysis method (Table II). From subgroup analysis of OS, the pooled HRs obtained from Kaplan-Meier curves and directly extracted from studies were 1.22 (95% CI: 1.05–1.39) and 1.41 (95% CI: 1.03–1.79), respectively, indicating that down-regulation of CDH1 was strongly correlated with poor OS. In the years after 2010, the Asia group, and age-based group ≥ 65 years old, the pooled HRs were 1.17 (95% CI: 1.00–1.35), 1.13 (95% CI: 0.93–1.33), and 1.15 (95% CI: 0.98–1.33), respectively, demonstrating that reduced expression of CDH1 had no significant correlation with OS.
Table II
Summarised hazard ratios of overall and subgroup analyses for overall survival in relation to E-cadherin expression in pancreatic cancer patients
Sensitivity analysis
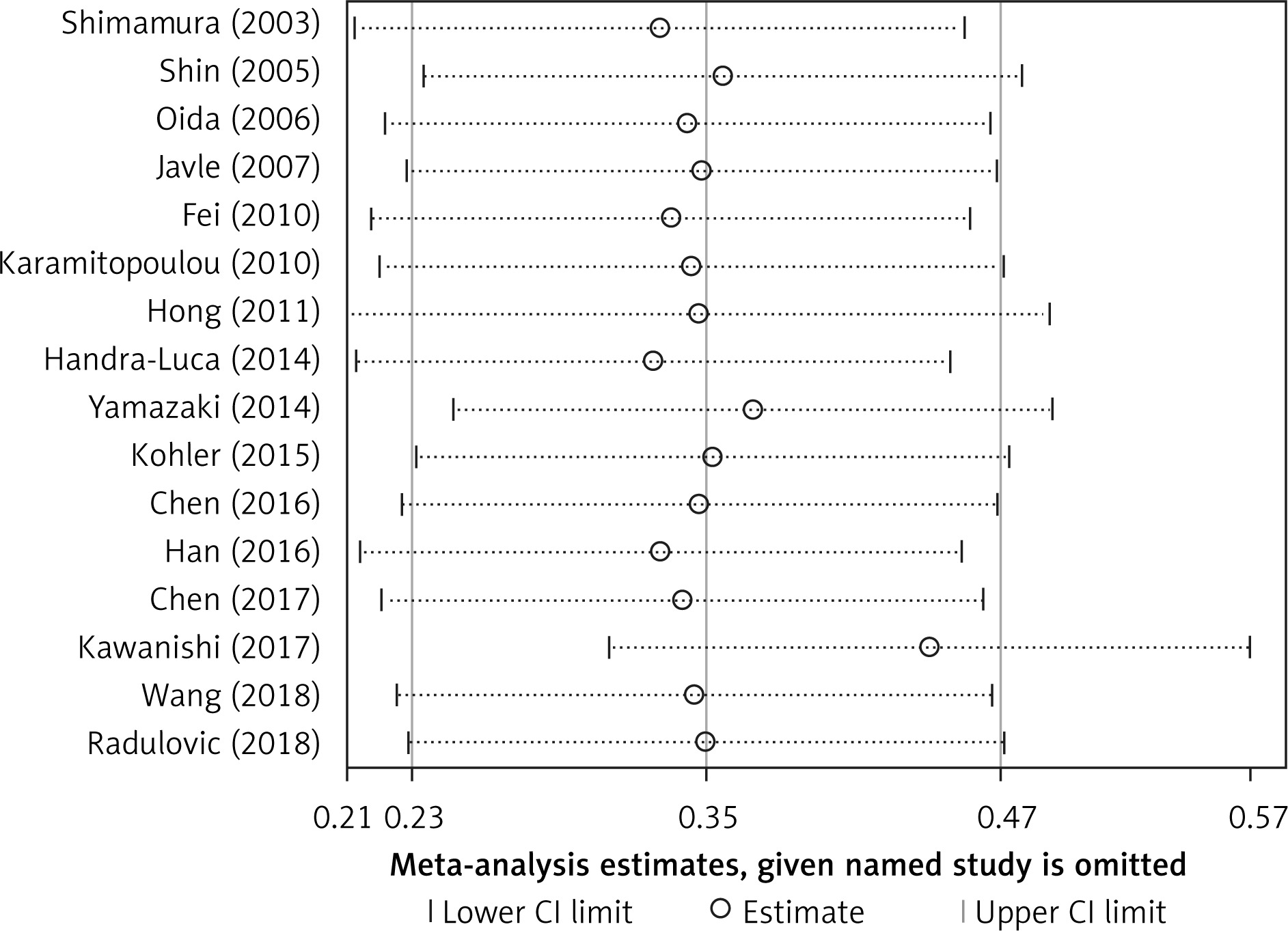
Sensitivity analysis was conducted as shown in Figure 3. The results revealed that the overall pooled HRs did not significantly change, suggesting that reduced expression of CDH1 predicting adverse OS among PC patients is reliable.
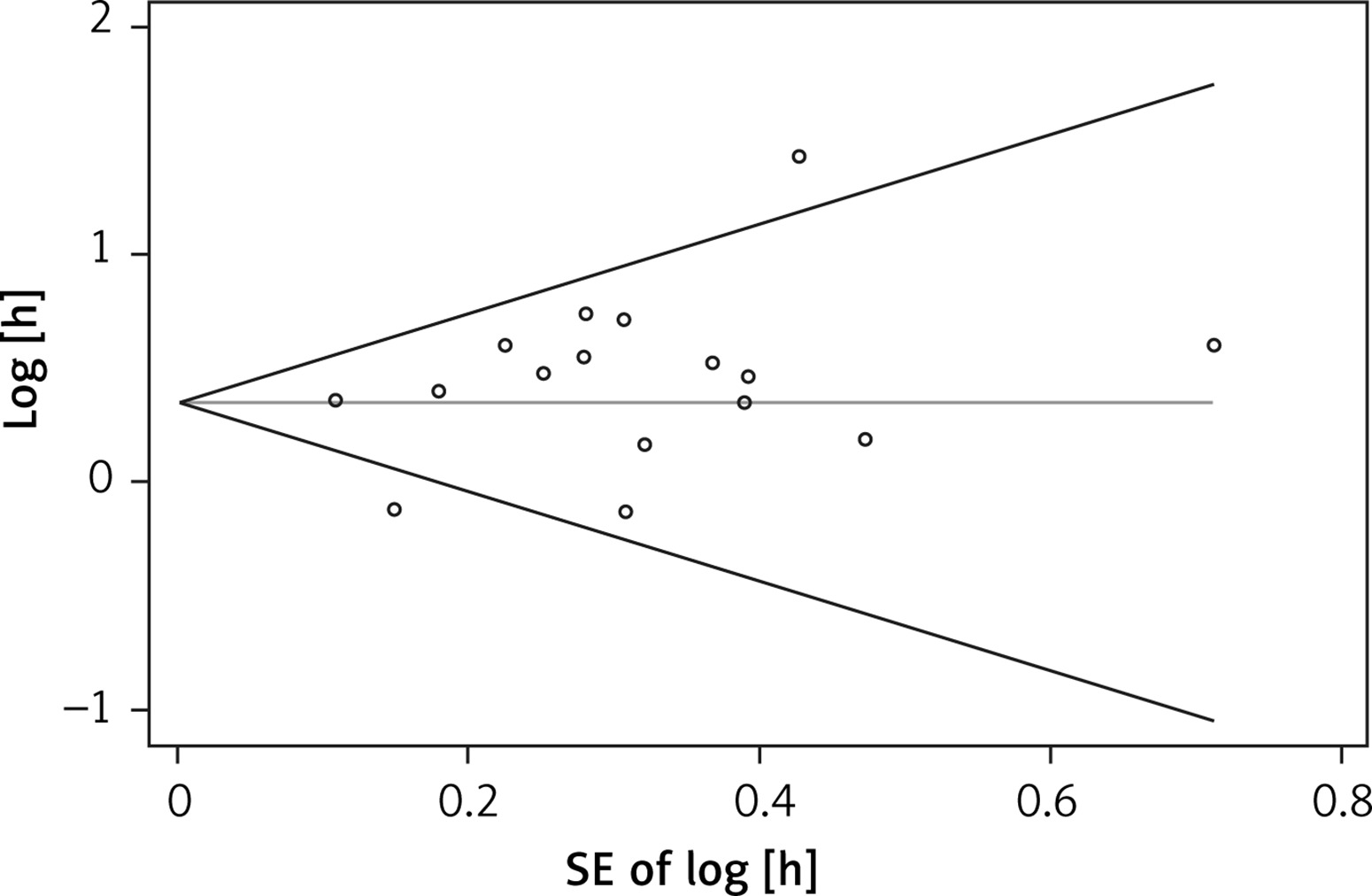
Publication bias
Egger’s test and Begg’s funnel plots (Figure 4) were applied to evaluate the publication bias for OS in PC patients. No significant publication bias was noted (OS: Egger’s test, p = 0.169; Begg’s test, p = 0.685).
Association of expression of CDH1 with clinicopathological features of PC patients
As shown in Table III, low-expression of CDH1 is dramatically associated with tumour grade (G1 vs. G2/G3, OR = 1.80, 95% CI: 1.07–3.03). However, there was no significant correlation between low-expression of CDH1 and age (≤ 60 vs. > 60 years old, OR = 0.85, 95% CI: 0.49–1.47), TNM stage (I/II vs. III/IV, OR = 1.78, 95% CI: 0.95–3.33), pathological T stage (T1/T2 vs. T3/T4, OR = 1.55, 95% CI: 0.10–2.42), lymph node (N1 vs. NO, OR = 0.81, 95% CI: 0.58–1.11), distant metastasis (M1 vs. M0, OR = 0.60, 95% CI: 0.23–1.53), vascular invasion (absent vs. present, OR = 0.88, 95% CI: 0.62–1.24) and tumour differentiation (well/moderate vs. poor, OR = 1.36, 95% CI: 0.96–1.92).
Table III
Meta-analysis of reduced expression of CDH1 and clinicopathological features of pancreatic cancer patients
Discussion
The cadherin superfamily is a major class of cell-cell adhesion molecules, cell surface glycoproteins that plays a substantial role in cell-cell adhesion, cancer, and tissue patterns [32–34]. Cell-cell adhesion determines cell polarity and participates in cell differentiation, in addition to the establishment and maintenance of tissue homeostasis. During oncogenesis, the organised adhesion is disturbed by genetic and epigenetic changes, leading to changes in signalling, loss of contact inhibition, and altered cell migration and stromal interactions. Related studies have showed that dysregulated cadherins are involved in different aspects of cancer progression, including cancer cell metastasis, invasion, drug resistance, and angiogenesis. Therefore, cadherins are considered as a potential therapeutic target, as well as being valuable diagnostic and prognostic indicators [7]. The classical cadherin family has more than 20 members, and epithelial CDH1 is the most widely studied member of the cadherin superfamily [8]. The most convincing data on the role of the cadherin family in cancer progression are also derived from CDH1 [7].
CDH1 has previously been described as a tumour suppressor molecule that significantly contributes to intercellular recognition, cell adhesion, and epithelial polarity in cancer [35]. It is also well known that CDH1 inhibits tumorigenicity and tumour dissemination by a complex mechanism that promotes apoptosis and tissue organisation. These mechanisms are involved in biophysical adhesion processes and intracellular signalling based on mechanical transduction [8, 35]. A number of scholars attempted to evaluate the prognostic significance of CDH1 expression in PC patients, but due to controversial results in published studies no consensus could be reached [11–13, 18, 19, 29, 31]. Therefore, we adopted stringent inclusion and exclusion criteria to conduct the meta-analysis.
A total of 1805 patients were incorporated into the current meta-analysis to find out the relationship between downregulated CDH1 expression and OS. The combined HR showed that reduced expression of CDH1 had adverse OS (HR = 1.25, 95% CI: 1.09–1.41) for PC patients, indicating that CDH1 is an independent prognostic marker for PC. No obvious heterogeneity was found in our meta-analysis. Furthermore, the reliability of the results was verified by subgroup analysis and sensitivity analyses. In subgroup analysis of OS, the pooled HRs obtained from Kaplan-Meier curves and directly extracted showed that decreased expression of CDH1 was significantly correlated with shorter OS. The present meta-analysis revealed the predictive value of CDH1 in Caucasian patients, in whom down-regulation of CDH1 was strongly correlated with poor OS. Conversely, in the subgroup analysis of Asian patients, downregulated expression of CDH1 did not indicate poor outcomes. The pancreas is an organ of the digestive system and endocrine system of vertebrates. Abnormal and uncontrolled growth of cells in the pancreas may result in pancreatic cancer. It has been estimated that about 90% of pancreatic cancer cases are due to environmental risk factors. Among them, approximately 50% of pancreatic cancer cases may be attributed to diet [36]. Environmental factors and the eating habit of different ethnicities could affect the prognostic function of CDH1; however, a great number of studies need to be conducted to verify this conclusion. In subgroup analysis of patients’ mean age, the heterogeneity of the group of < 65 years old group was 0%, while the group ≥ 65 years old had significant heterogeneity (I2 = 40.80%). A potential factor is that, in the < 65 group, low expression of CDH1 was significantly correlated with overall survival, which means that, the group < 65 years old was more objective and clinically significant compared with group ≥ 65 years old.
In the present meta-analysis, we performed a comprehensive analysis to explore the influence of reduced expression of CDH1 on clinicopathological parameters. Our meta-analysis showed that reduced expression of CDH1 was associated with tumour grade, excluding TNM staging, age, distant metastasis, pathological T stage, tumour differentiation, vascular invasion, and lymph node metastasis. Numerous factors might affect the results, such as the small number of patients, multiple treatments, as well as missing clinical and pathological data. The clinical-pathological parameters of a variety of studies have not been reported; thus, further studies need to be conducted to confirm the correlation between CDH1 expression and clinical-pathological parameters.
Our meta-analysis has a number of limitations. First, the language of the studies included in this meta-analysis was limited to English, and the retrieval strategy was restricted to two databases (PubMedand and EMBASE). It is possible that other potentially relevant studies, which meet our inclusion criteria, cannot be identified. Second, primary antibodies from different sources may result in discrepancies in IHC sensitivity, without universal scoring criteria to define the reduced expression of CDH1. Third, the survival analysis was not performed by multivariate analyses in many of the included studies; we therefore estimated the HR from Kaplan-Meier curves, which lacked reliability due to the inaccurate calculation of the censored data. Forth, we eliminated some research with no statistical significance, because effective data could not be obtained to calculate HRs. Fifth, in our meta-analysis, the final results indicated that CDH1 expression was negatively correlated with adverse OS, with low heterogeneity (I2 = 27.1%, p = 0.151). We did not further find the cause of heterogeneity through meta regression. Furthermore, the majority of the studies included in this meta-analysis lacked clinical and pathological characteristics of tumours. The variables could introduce heterogeneity or affect the analyses performed.
In conclusion, this meta-analysis demonstrated that reduced expression of CDH1 can predict OS for PC patients. Additionally, the CDH1 was negatively correlated with tumour grade. According to our results, the expression of CDH1 may provide incremental OS prognostic data, and it may be used as a promising prognostic biomarker for patients with PC. These insights may promote effective strategies for therapeutic intervention of PC. However, further high-quality and large-scale clinical studies are required to validate our findings.