Introduction
The HER2/neu (ERBB2) oncogene is increased in copy number and/or overexpressed in about 15–20% of breast cancers (BC) and serves as a significant prognostic marker for relapse and poor overall survival (OS) [1]. However, the development of anti-HER2 therapies has improved the prognosis for patients with both advanced and early-stage HER2-positive breast cancer [2–4].
Breast cancer is categorized into four distinct subtypes based on hormone receptor (HR) and human epidermal growth factor receptor 2 (HER2) status: HR+/HER2−, HR+/HER2+, HR−/HER2+, and HR−/HER2 [5]. In medical practice, international guidelines divide BC into HER2-positive (HER2+) and HER2-negative (HER2−) categories to inform treatment decisions [6]. HER 2 overexpression is assessed as HER2-zero, HER2 IHC1+, HER2 IHC2+/ISH-negative, HER2 IHC2+/ISH-positive, and HER2 IHC3+. HER2 positivity is defined as an IHC score of 3+ or 2+ with in situ ISH amplification [7]. Recent studies have proposed a novel subgroup of breast cancers called “HER2-low breast cancer”, defined by an IHC score of 1+ or 2+ without ISH amplification [8, 9]. In clinical settings, these tumors were not considered candidates for anti-HER2 therapies. Two-thirds of HR-positive tumors and one-third of triple-negative tumors exhibit low HER2 expression in immunohistochemistry (IHC) [10]. Earlier research has demonstrated that HER2-low breast cancers are more frequently associated with HR-positive (HR+) status, lower tumor grade, lower Ki67, and a higher proportion of invasive lobular carcinoma [11, 12].
Some studies have assessed the prognostic value of HER2-low status in breast cancer patients [10, 13–19]. Moreover, distinct survival patterns and clinicopathological characteristics have also been reported between HER2-low IHC 1+ and HER2-low IHC 2+w/ISH-negative subgroups [13, 20, 21].
The purpose of this study was to assess the prognostic importance of HER2-low status in BC. We also compared the HER2-low (HER2-low1+; HER2-low2+/ISH(-)) subgroup with HER2-zero and HER2-positive subgroups in terms of clinical, histopathological, and molecular factors.
Material and methods
Patients
The retrospective study was carried out on a cohort of 657 female patients diagnosed with BC treated at the Maria Sklodowska-Curie National Research Institute of Oncology (Gliwice Branch) between 2002 and 2018. Demographic data, such as age, menopausal status, and family history, as well as tumor characteristics including histology, estrogen receptor (ER) and progesterone receptor (PR) status, HER2 status (including both IHC and ISH results), Ki67, and disease stage according to the TNM staging system (T – tumor size; N – nodal involvement; and M – metastasis) were collected from hospital medical files and pathology reports. Additional data included the presence of contralateral breast cancer and details regarding the treatment strategy, including surgical procedures, systemic treatment, or radiotherapy. The analysis of patient medical records was conducted in compliance with domestic legal regulations. All patients in this study were treated following the latest standard guidelines for chemotherapy and radiotherapy, irrespective of their HER2 status. Patients continue to undergo regular follow-up at the cancer research center. The complete overview of patients’ demographic and clinicopathological characteristics is presented in Table I.
Table I
Patients’ characteristics and comparison of subgroups according to clinicopathological factors
| Parameter | HER2-zero (N = 248 (100%)) | HER2-low (N = 176 (100%)) | HER2-positive (N = 233 (100%)) | P-value | HER2-zero vs HER2-low P-value* | HER2-low vs HER2-positive P-value* |
|---|---|---|---|---|---|---|
| Age [years] (mean ± SD) | 51.2 ±10.98 | 52.4 ±11.12 | 52.2 ±10.53 | 0.485 | 0.825 | 0.514 |
| Family history of cancer | 113 (45.6%) | 72 (40.9%) | 102 (43.8%) | 0.637 | 1.00 | 0.921 |
| Comorbid condition | 77 (31.0%) | 71 (40.3%) | 80 (34.3%) | 0.141 | 0.151 | 0.325 |
| Postmenopausal status | 118 (47.6%) | 87 (49.4%) | 116 (49.8%) | 0.889 | 1.00 | 1.000 |
| Tumor size T3-T4 | 41 (16.5%) | 29 (16.5%) | 53 (23.2%) | 0.157 | 1.00 | 0.202 |
| Lymph nodes N+ | 82 (33.1%) | 58 (33.0%) | 129 (55.4%) | < 0.001 | 1.00 | 0.000 |
| Histologic tumor grade G3 | 77 (31.0%) | 47 (26.7%) | 96 (41.2%) | 0.005 | 0.386 | 0.002 |
| Estrogen receptor positive ER+ | 147 (59.3%) | 141 (80.1%) | 149 (63.9%) | < 0.001 | < 0.001 | 0.001 |
| Progesterone receptor positive PR+ | 137 (55.2%) | 134 (76.1%) | 127 (54.5%) | < 0.001 | < 0.001 | < 0.001 |
| Hormone receptor positive HR+ | 154 (62.1%) | 145 (82.4%) | 149 (63.9%) | < 0.001 | < 0.001 | < 0.001 |
| BRCA mutation | 37 (14.9%) | 24 (13.6%) | 2 (0.9%) | < 0.001 | 0.780 | < 0.001 |
| CHEK2 | 17 (6.9%) | 16 (9.1%) | 8 (3.4%) | 0.050 | 0.463 | 0.058 |
| Ductal carcinoma | 175 (70.6%) | 126 (71.6%) | 196 (84.1%) | < 0.001 | 0.825 | 0.003 |
| Lobular carcinoma | 34 (13.7%) | 23 (13.1%) | 10 (4.3%) | |||
| Other histological types | 39 (15.7%) | 27 (15.3%) | 27 (11.6%) | |||
Hormone receptor and HER2 classification
Human epidermal growth factor receptor 2 (HER2) overexpression was evaluated by means of an immunohistochemistry (IHC) in postoperative specimens or in samples collected via core needle biopsy. Patients’ HER2 status was categorized as 0, + 1, + 2, or + 3 according to IHC results. Scores of 0, + 1, and + 3 represent HER2-zero, HER2-low, and HER2-positive, respectively. For cases with IHC 2+, additional testing for HER2 gene amplification was conducted using fluorescence in situ hybridization (FISH). HER2 expression was assessed using IHC and ISH based on the latest version of the American Society of Clinical Oncology/College of American Pathologists Clinical Practice (ASCO/CAP) guidelines available on the day of surgery [7]. In summary, HER2-low was classified as IHC 1+ (HER2-low1+) and IHC 2+ with negative ISH (HER2-low2+/ISH(-)). HER2-zero was defined as IHC 0, while scores of 3+ or 2+/ISH+ correspond to HER2-positive status. Tumor samples with more than 1% of tumor nuclei positive for estrogen receptor (ER) or progesterone receptor (PR) were classified as ER/PR positive. Hormone receptor (HR) positivity was defined as the presence of ER and/or PR positivity [22].
Statistical analysis
Statistical analysis was carried out using Statistica 13.1 (TIBCO Software Inc.). Categorical variables were presented as frequencies and percentages. Fisher’s exact test was used to compare patient subgroups, with the Benjamini-Hochberg correction applied to address multiple comparisons. Statistical significance was determined by a p-value < 0.05. Survival curves were determined with the Kaplan-Meier method, and comparisons between groups were performed using the log-rank test. Confounding and effect-modifying variables were studied through multivariate analysis. The Cox proportional hazards model was applied for both univariate and multivariate analysis to assess the impact of selected variables on OS. Variables with a p-value < 0.200 were included in the multivariate analysis.
Results
Patient characteristics
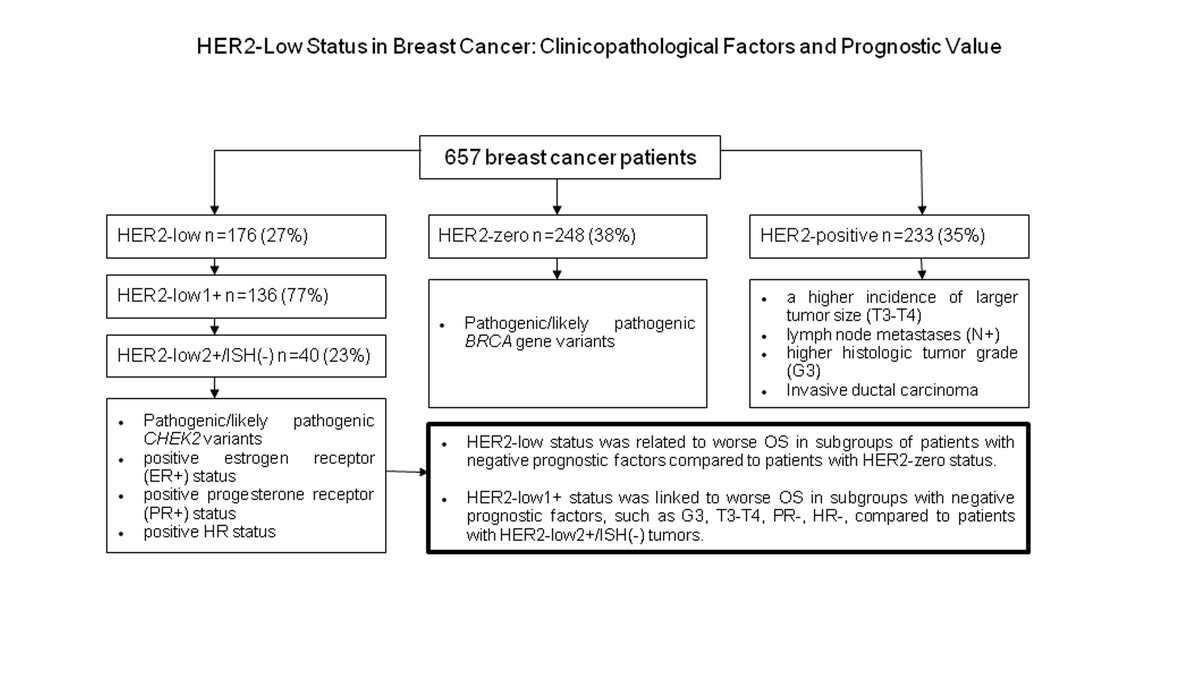
The median age of all patients was 52 years (range: 24 to 81 years). Among the tumors, 176 (27%) were classified as HER2-low, 248 (38%) as HER2-zero, and 233 (35%) as HER2-positive. Within the HER2-low group, 136 tumors were categorized as HER2-low1+ and 40 as HER2-low2+/ISH(-). No significant differences were reported between the three subgroups (HER2-zero; HER2-low; HER2-positive) concerning family history of cancer, co-existing medical conditions, and menopausal status. Patients with HER2-positive tumors had a higher incidence of larger tumor size (T3-T4) (23.2%), lymph node metastases (N+) (55.4%) and higher histologic tumor grade (G3) (41.2%). However, positive estrogen receptor (ER+) status (80.1%), positive progesterone receptor (PR+) status (76.1%), and positive HR status (82.4%) were more often reported in patients with HER2-low tumors. Invasive ductal carcinoma was more common in patients with HER2-positive tumors versus those with HER2-low and HER2-zero tumors (84.1% vs. 71.6% vs. 70.6%; p < 0.001). Pathogenic/likely pathogenic BRCA gene variants were substantially more prevalent in subjects with HER2-zero tumors (14.9%, p < 0.001). On the other hand, pathogenic/likely pathogenic CHEK2 variants were more frequently observed in patients with HER2-low tumors versus those with HER2-positive and HER2-zero tumors (9.1% vs. 3.4% vs. 6.9%; p = 0.050). Patient characteristics according to clinicopathological factors are shown in Table I.
Comparison of HER2-low tumors with HER2-zero breast cancer
There were no significant differences in molecular factors, including BRCA gene mutations (p = 0.780) or age (p = 0.825), between subjects with HER2-low tumors and HER2-zero tumors. Similarly, no differences were observed between the two groups with respect to family history of cancer (p = 1.00), comorbid conditions (p = 0.151), menopausal status (p = 1.00), tumor size (T3-T4) (p = 1.0), lymph node metastases (N+) (p = 1.0), or histologic tumor grade (G3) (p = 0.386). However, BC patients with HER2-low tumors more frequently had positive estrogen receptor (ER+) status (80.1% vs. 59.3%, p < 0.001) and progesterone receptor (PR+) status (76.1% vs. 55.2%, p < 0.001) compared to patients with HER2-zero tumors. There was also a notable difference between the two groups regarding combined hormone receptor (HR+) (82.4% vs. 62.1%, p < 0.001) (Table I).
BC subjects with HER2-low1+ tumors were more likely to have positive hormone receptor (HR+) status compared to those with HER2-zero tumors (82.4% vs. 62.1%, p < 0.001). Specifically, ER+ status was observed in 80.9% of patients with HER2-low1+ tumors compared to 59.3% in HER2-zero patients (p < 0.001), and PR+ status was observed in 74.3% of HER2-low1+ patients compared to 55.2% in the HER2-zero group (p < 0.001). Similar results were obtained for the subgroup with HER2-low2+/ISH(-) tumors, where patients also more frequently had positive HR status versus those with HER2-zero tumors (82.5% vs. 62.1%, p = 0.025).
In total, 94 tumors were classified as TNBC HER2-zero, while 24 tumors were HER2-low1+ and 7 tumors were HER2-low2+/ISH(-). No significant differences were noted between TNBC HER2-zero and TNBC HER2-low1+ with respect to comorbid conditions (p = 0.657), menopausal status (p = 1.00), tumor size (T3-T4) (p = 1.00), lymph node metastases (p = 0.629), or histologic tumor grade (G3) (p = 1.00). Similarly, there were no differences between TNBC HER2-zero and HER2-low2+/ISH(-) tumors according to the above mentioned factors.
Comparison of HER2-low tumors with HER2-positive breast cancer
Significant differences were reported between HER2-low and HER2-positive tumors regarding ER+ (80.1% vs. 63.9%, p < 0.001), PR+ (76.1% vs. 54.5%, p < 0.001), HR+ (82.4% vs. 63.9%, p < 0.001), and the invasive ductal carcinoma (IDC) subtype (71.6% vs. 84.1%, p = 0.003). BRCA pathogenic/likely pathogenic variants were more common in patients with HER2-low breast cancer compared to HER2 positive tumors (13.6% vs. 0.9%, p < 0.001). Similarly, CHEK2 pathogenic/likely pathogenic variants were noted more often in the HER2-low subtype compared to HER2-positive tumors (9.1% vs. 3.4%, p = 0.058) (Table I).
Lymph node metastases (N+) were detected more frequently in patients with HER2-positive tumors versus those with HER2-low1+ tumors (55.4% vs. 34.6%, p < 0.001) and HER2-low2+/ISH(-) tumors (55.4% vs. 27.5%, p = 0.004). BC patients with HER2-low1+ tumors more frequently had positive hormone receptor (HR+) status compared to HER2-positive tumors (82.4% vs. 63.9%, p = 0.003). In addition, patients with HER2-low2+/ISH(-) more frequently had positive HR status compared to HER2-positive status (82.5% vs. 63.9%, p = 0.042). In contrast, negative progesterone receptor status was more often reported in the HER2-positive subgroup compared to HER2-low1+ (p = 0.001) and HER2-low2+/ISH(-) (p = 0.002) groups. A higher histological tumor grade (G3) was reported more frequently in subjects with HER2 positive tumors compared to HER2-low 1+ breast cancer (41.2% vs. 27.2%, p = 0.043) or HER2-low2+/ISH(-) (41.2% vs. 25.05, p = 0.111).
Comparison of HER2-low1+ tumors with HER2-low2+/ISH(-) breast cancer
No difference was found between the HER2-low1+ tumors and HER2-low2+/ISH(-) subgroups regarding positive hormone receptor (HR+) status (82.4% vs. 82.5%, p = 1.00). Similarly, no differences were detected between the two subgroups regarding family history of cancer (40.4% vs. 42.5%, p = 1.00), comorbid conditions (42.6% vs. 32.5%, p = 0.552), menopausal status (47.8% vs. 55.0%, p = 1.00), tumor size T3-T4 (16.9% vs. 15.0%, p = 1.00), lymph node metastases (N+) (34.6% vs. 27.5%, p = 0.674), or higher histologic tumor grade (G3) (27.2% vs. 25.0%, p = 0.842). Additionally, no difference was found between the two subgroups regarding the existence of BRCA pathogenic or probably pathogenic variants (16.2% vs. 5.0%, p = 0.169). In contrast, the occurrence of CHEK2 pathogenic or probably pathogenic variants was reported more frequently in patients with HER2-low2+/ISH(-) than in the HER2-low1+ subgroup (20.0% vs. 5.9%, p = 0.034) (Table II).
Table II
Comparison of HER2-low1+ and HER2-low2+/ISH(-) breast cancer
| Parameter | HER2-low1+ N = 136 (100%) | HER2-low2+/ISH(-) N = 40 (100%) | P-value* |
|---|---|---|---|
| Age [years] (mean ± SD) | 52.5 ± 11.0 | 52.3 ± 11.6 | 1.00 |
| Family history of cancer | 55 (40.4%) | 17 (42.5%) | 1.00 |
| Comorbid condition | 58 (42.6%) | 13 (32.5%) | 0.552 |
| Postmenopausal status | 65 (47.8%) | 22 (55.0%) | 1.00 |
| Tumor size T3-T4 | 23 (16.9%) | 6 (15.0%) | 1.00 |
| Lymph nodes N+ | 47 (34.6%) | 11 (27.5%) | 0.674 |
| Histologic tumor grade G3 | 37 (27.2%) | 10 (25.0%) | 0.842 |
| Estrogen receptor positive ER+ | 110 (80.9%) | 31 (77.5%) | 0.655 |
| Progesterone receptor positive PR+ | 101 (74.3%) | 33 (82.5%) | 0.478 |
| Hormone receptor positive HR+ | 112 (82.4%) | 33 (82.5%) | 1.00 |
| BRCA mutation | 22 (16.2%) | 2 (5.0%) | 0.169 |
| CHEK2 | 8 (5.9%) | 8 (20.0%) | 0.034 |
Similarly, no differences were found between HER2-low1+ ER positive tumors and HER2-low2+/ISH(-) ER positive tumors regarding factors such as family history of cancer (39.1% vs. 41.9%, p = 1.00), comorbid conditions (44.5% vs. 32.3%, p = 1.00), menopausal status (49.1% vs. 58.1%, p = 1.00), tumor size (T3-T4) (13.6% vs. 12.9%, p = 1.00), lymph node metastases (33.6% vs. 29.0%, p = 1.00), histologic tumor grade (G3) (20.0% vs. 25.8%, p = 0.701), and positive progesterone receptor status (90% vs. 100%, p = 0.122). Also, no differences were observed between HER2-low1+ ER negative tumors and HER2-low2+/ISH(-) ER negative tumors according to the same factors.
In contrast, statistically significant differences were found between HER2-low1+ ER positive tumors and HER2-low1+ ER negative subgroups with regard to histologic tumor grade (G3) (20.0% vs. 57.7%, p < 0.001) and PR+ (90.0% vs. 7.7%, p < 0.001). PR+ status was observed more frequently in ER+ HER2-low2+/ISH(-) tumors compared to the ER- HER2-low2+/ISH(-) subgroup (100% vs. 22.2%, p < 0.001).
Overall survival outcomes
No difference was observed in OS between patients with HER2-low and HER2-zero status (p = 0.747). In the subgroup of patients with ER-negative receptor status (ER-), OS was slightly worse for those with HER2-low status compared to those with HER2-zero status, although the difference was not statistically significant (5-year OS 72.6% vs. 86.7%, p = 0.074) (Figure 1 A). No difference in OS was also observed in the subgroup with ER-positive status (p = 0.763). The occurrence of lymph node metastases (N+) was found to be similar between the two groups of patients (81.3% vs. 86.9%, p = 0.599). Non-significantly worse OS was noted in patients with HER2-low status within subgroups showing higher T3-4 (61.2% vs. 75.1%, p = 0.217) and G3 (80.7% vs. 89.2%, p = 0.139).
Figure 1
Overall survival outcomes in breast cancer patients according to HER2 status: HER2-zero vs. HER2-low (A) and HER2-zero vs. HER2-low1+ (B–D)
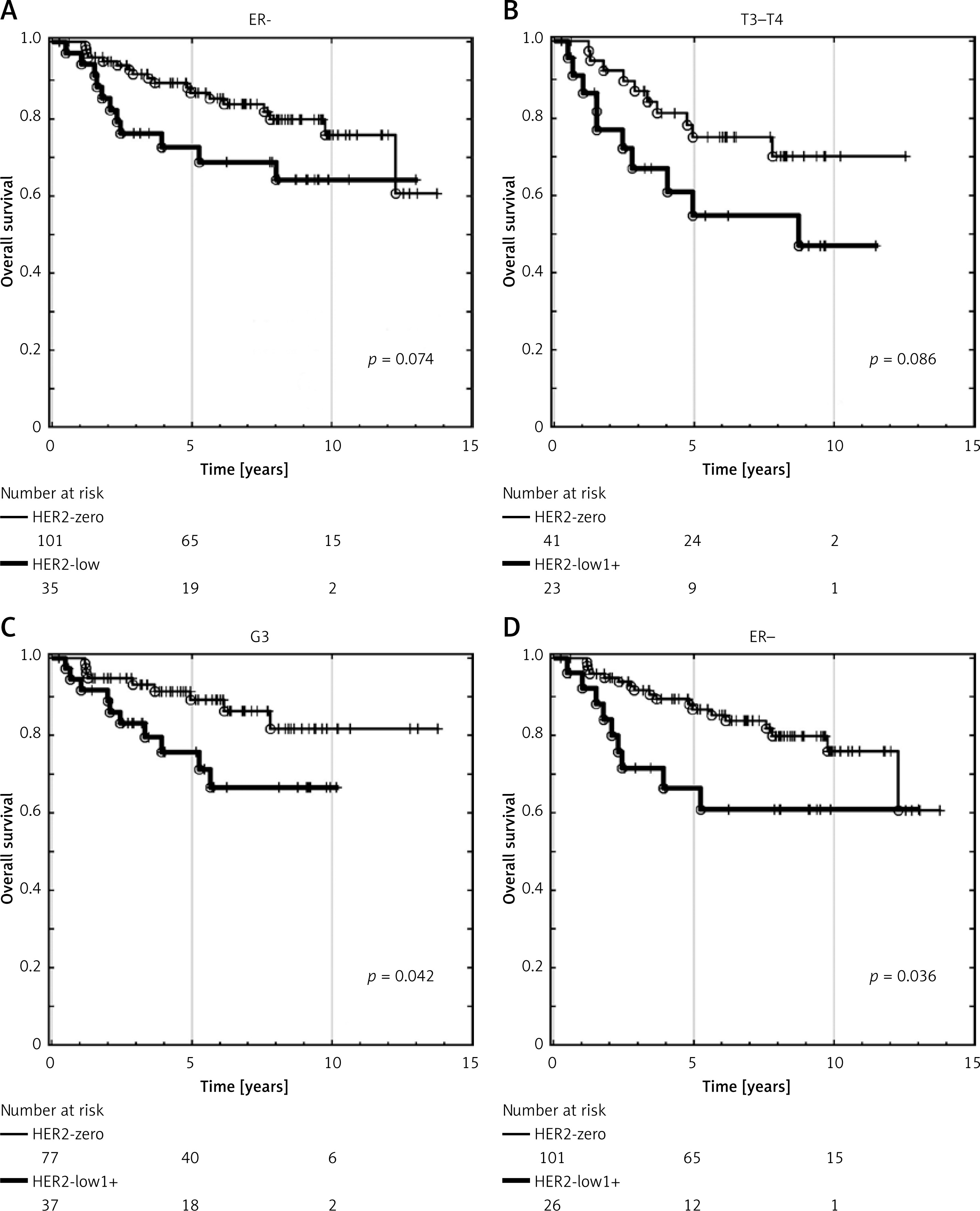
For patients with HER2-low1+ status, no significant difference in OS was observed versus those with HER2-zero status (p = 0.701). In the subgroup of patients with HR-negative receptor status (HR-) (p = 0.191), OS was insignificantly poorer for those with HER2-low1+ compared to the HER2-zero group. Non-significantly worse OS was observed in HER2-low1+ patients with larger tumor sizes (T3-T4) (p = 0.086) (Figure 1 B). However, in patients with G3 (p = 0.042) (Figure 1 C) and negative estrogen receptor status (p = 0.036) (Figure 1 D), OS was significantly poorer in the HER2-low1+ subgroup.
There was no significant difference in OS between patients with HER2-low2+/ISH(-) and HER2-zero tumors (p = 0.967). Non-significantly better OS was noted in patients with HER2-low2+/ISH(-) in subgroups with negative progesterone receptor status (p = 0.132) and negative HR receptor status (p = 0.161). No differences in OS were found between patients with HER2-low2+/ISH(-) and HER2-zero in subgroups with T3-T4 (p = 0.513), G3 (p = 0.341), and ER- (p = 0.883).
There was no significant difference in OS between patients with HER2-low1+ and HER2-low2+/ISH(-) status (p = 0.778). In the subgroup of patients with HR negative receptor status (HR-) (p = 0.089) (Figure 2 A), OS was slightly worse in patients with HER2-low1+ status compared to HER2-low2+/ISH(-). Non-significantly worse OS was noted in HER2-low1+ patients within subgroups with negative progesterone receptor status (p = 0.110), G3 (p = 0.090) (Figure 2 B), and tumor size T3-T4 (p = 0.128).
Figure 2
Overall survival outcomes in breast cancer patients according to HER2 status: HER2-low2+/ISH(-) vs. HER2-low1+ (A, B) and HER2-positive vs. HER2-low (C, D)
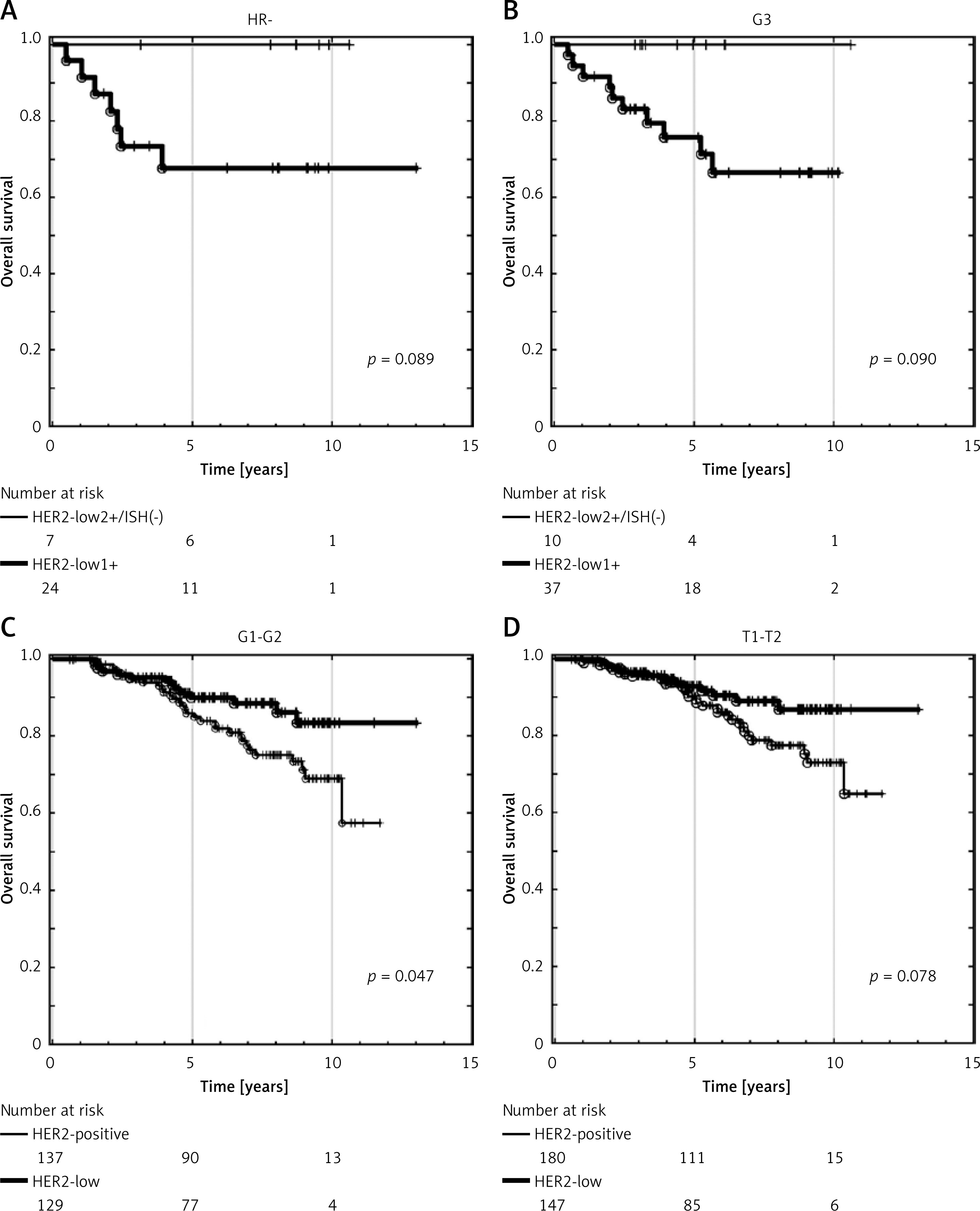
Patients with HER2-low tumors showed non-significantly better OS compared to the HER2-positive subgroup (p = 0.144). In subgroups with histological grade G1-2 (p = 0.047) (Figure 2 C), OS was significantly better in the HER2-low subgroup, while in subgroups with T1-T2 (p = 0.078) (Figure 2 D), OS was slightly better in the HER2-low subgroup. Non-significantly better OS was also noted in patients in the HER2-low subgroups with PR positive (p = 0.139) and ER positive (p = 0.220) receptor status.
Univariate analysis revealed several factors associated with poorer OS, including age over 60 years, higher T (T3-4), and the existence of lymph node metastases (N+). Similarly, HER2-positive breast cancer was associated with significantly worse OS versus HER2-zero subtypes. In contrast, both ER-positive and PR-positive statuses were associated with better OS. Multivariate analysis confirmed the independent influence of factors such as age over 60 years, T3-T4, N+, and ER and PR status on OS, suggesting that HER2 expression does not significantly impact OS results (Table III).
Table III
Univariate and multivariate analysis
The strengths of this study include a follow-up time for survival events longer than 5 years (ranging from 7 to 13 years), relatively complete data in our database, and consideration of certain genetic factors. However, this study has also some limitations. It was a single-center and retrospective analysis, which limits the generalizability of results. Additionally, the number of patients in some subgroup evaluations was small, potentially affecting the statistical power of the analysis.
Discussion
In this study, we evaluated the clinical, histological, and survival characteristics of HER2-low breast cancer patients, as well as HER2-zero and HER2-positive subgroups in a cohort of 657 patients. Of these, 176 (27%) tumors were defined as HER2-low breast cancer. The HER2-low group included 136 subjects with HER2-low1+ and 40 patients with HER2-low2+/ISH(-) status. In previous studies, the HER2-low subgroup has constituted around 30-50% of the total research population [23–25].
Consistent with previous research [13, 18, 26–29], our study revealed a significantly higher frequency of hormone receptor (HR) status positivity (ER and PR) in the HER2-low group compared to the HER2-zero and HER2-positive subgroups. Specifically, HER2-low tumors were more likely to be HR positive than HER2-zero or HER2-positive tumors. In the literature, the HER2-low subgroup is related to less aggressive clinicopathological characteristics, such as a lower prevalence of grade 3 tumors, a lower Ki67 index, and a smaller number of TP53 mutations. This suggests that HER2-low tumors more closely resemble HER2-negative than HER2-positive tumors [13]. Petrelli et al. also observed more favorable prognostic factors in HER2-low patients, such as lower Ki67%, more ER-positive cases, and a higher proportion of grade 2 tumors versus HER2 IHC 0 [10]. Similarly, Yang et al. reported a lower incidence of histological grade III cases (29.4% vs. 38.8%, p < 0.001) and a greater percentage of HR-positive cases (89.6% vs. 75.6%, p < 0.001) in HER2-low tumors versus HER2-zero tumors [16]. Yang et al. found that HER2-low breast cancer was strongly associated with increased HR and AR expression, as well as a lower Ki67 index [30]. Similar results were observed in a study conducted by Sato et al. Their analysis showed that the presence of HER2-low breast cancer was significantly associated with HR-positive status and a lower median Ki-67 compared to HER2-negative patients [28]. Additionally, clinicopathological characteristics such as ductal adenocarcinomas histology and hormone receptor positivity were more frequently reported by Khalil et al. [27]. A combined analysis of four prospective neoadjuvant clinical trials with 2,310 subjects revealed that HER2-low breast cancers were more commonly HR-positive, had lower histological grades (I and II), and displayed a reduced Ki-67 labeling index [25]. Additional research has linked the HER2-low group with non-IDC histotypes and a tendency for absence of necrosis [31]. However, in a study by de Nonneville et al., no significant differences were found regarding patient age, clinical T and N stages, pathological type, type of breast surgery, or type of surgical axillary surgery between HER2-low and HER2-0 tumors. HER2-low status was, however, independently associated with HR positivity [32]. Schettini et al. and Agostinetto et al. have shown that HER2-low breast cancers constitute a heterogeneous group based on molecular subtypes. They reported that luminal A (50.8–56.9%) and luminal B (22.8–28.8%) subtypes were most prevalent, followed by basal-like (13.3–17.7%) and HER2-enriched (3.5–3.6%) subtypes [14]. Zhang et al. reported a similar distribution, with luminal B (58.9–76%) and luminal A (20–28.6%) being the most frequent subtypes [33]. These studies reported a high occurrence of luminal subtypes and fewer HER2-enriched and basal-like subtypes in HR+/HER2-low tumors [14, 33, 34]. However, no significant association between clinical and pathological factors and HER2-low status in male breast cancer (MBC) was reported [35]. The Expert Consensus Statements by the European Society for Medical Oncology (ESMO) suggest that HER2-low tumors should be considered a heterogeneous group of tumors rather than a distinct molecular entity [36].
In our study, there were no differences in molecular factors such as BRCA gene mutations, patient age, family cancer history, co-existing conditions, menopausal status, tumor size (T3-T4), lymph node metastasis (N+), or higher histological grade (G3) between patients with HER2-low and HER2-zero tumors. HR positivity was more common in patients with HER2-low tumors. Invasive ductal carcinoma was more frequently reported in female patients with HER2-positive tumors compared to HER2-low and HER2-zero status. Pathogenic/likely pathogenic BRCA gene variants were characteristic of patients with HER2-zero tumors, while pathogenic/likely pathogenic CHEK2 variants were more common in HER2-low tumors than in either HER2-positive or HER2-zero tumors.
Li et al. reported that HER2-low TNBC was associated with a lack of necrosis and a higher pN stage. The characteristics of the HER2-low group were assessed based on the HR status, younger age, and smaller tumor size [31]. HER2-low breast cancer was more commonly reported in patients with HR-positive status than in those with TNBC. HER2-low TNBC was characterized by a high lymph node ratio and positive lymphatic invasion [37]. Da Silva et al. found that in early-stage TNBC, the clinicopathological and demographic characteristics of the HER2-low subgroup did not differ significantly from those of the HER2-zero subgroup. Similarly, no significant differences were found in the recurrence-free survival (RFS), event-free survival (EFS), or OS between these subgroups [38]. No significant differences were noted in clinicopathological factors between HER-low and HER2-zero TNBC tumors.
Abbasvandi et al. reported that HER2-low female patients revealed the highest disease-free survival (DFS) and OS among the entire patient cohort. The differences in survival outcomes between the HER2-low and HER2-positive groups were significant, while those between HER2-low and HER2-negative patients were not statistically significant [13]. HER2 IHC 2+/ISH negative breast cancers had substantially better DFS versus HER2-negative patients. Nevertheless, no differences in DFS were reported between HER2-low IHC 1+ and HER2-negative tumors [13]. In contrast, other analyses showed that HER2-low IHC2+/ISH negative early-stage BC had worse DFS compared to HER2 IHC 0 or 1+ patients [20, 21]. Additionally, worse DFS was reported in subjects with HER2-low status and lobular breast cancer versus HER2-negative tumors [10].
Molinelli et al. conducted a systemic literature review to determine research comparing survival outcomes in breast cancer patients with HER2-low status versus HER2-0 status [39]. HER2-low status appeared to be associated with a slightly improved OS in both the advanced and early breast cancer, irrespective of hormone receptor expression, when compared to HER2-zero status. In early-stage breast cancer, HER2-low status was associated with significantly better DFS (HR = 0.86, 95% CI: 0.79–0.92, p < 0.001) and OS (HR = 0.90, 95% CI: 0.85–0.95, p < 0.001) versus HER2-zero status. Better OS was observed in both hormone receptor-positive and hormone receptor-negative HER2-low subgroups, with higher DFS found only in the hormone receptor-positive group. HER2-low status was significantly associated with a lower rate of pathological complete response (pCR) compared to HER2-zero status, both in the overall population (OR = 0.74, 95% CI: 0.62–0.88, p = 0.001) and in the hormone receptor-positive subgroup (OR = 0.77, 95% CI: 0.65–0.90, p = 0.001). In metastatic breast cancer, patients with HER2-low tumors had better OS compared to those with HER2-zero tumors in the overall population (HR = 0.94, 95% CI: 0.89–0.98, p = 0.008), regardless of hormone receptor status, although no significant differences in progression-free survival (PFS) were observed. [39]. Yang et al. found that low HER2 expression was related to a prolonged recurrence-free interval (RFI) in breast cancer patients, especially in HR-positive breast cancer patients (p = 0.028) and < 65-year-old breast cancer patients (p < 0.001) [16]. In early-stage TNBC, HER2-low expression was associated with better breast cancer-specific survival (BCSS) than those with the HER2-0 status (96.6% vs. 93.7%; log-rank p = 0.027). Among stage III patients, both BCSS and OS were better in the HER2-low subgroup versus the HER2-0 subgroup (BCSS, log-rank p = 0.010; OS, log-rank p = 0.047), though similar results were not observed in patients with stages I and II [40]. Zattarin et al. reported that HER2-low status was associated with worse PFS and OS in patients with HR-positive/HER2-negative advanced breast cancer (aBC) treated with first-line endocrine therapy plus CDK4/6i [41]. In another study, the risk of progression and/or death was greater in patients with HER2-low tumors compared to those with HER2-zero tumors (HR = 1.22, 95% CI: 1.10–1.35, p < 0.001). A combined analysis of several studies indicated that the risk of death was also higher in the HER2-low group compared to the HER2-zero group (HR = 1.22, 95% CI: 1.04–1.44, p = 0.010) [42]. However, in a study conducted by Yang et al., no significant difference was found between HER2-0 and HER2-low groups in either DFS or distant DFS (DDFS) [30]. A landmark analysis indicated that patients with HR-positive/HER2-low tumors had better DFS compared to the HR-positive/HER2-zero subgroup after 5 years. HER2-low expression was identified as an independent prognostic factor for DFS following 5 years, with a 69% reduced risk compared to HER2-zero expression (HR = 0.31, 95% CI: 0.13–0.75, p = 0.01). However, similar outcomes were not observed in terms of OS for HR-positive patients. No significant difference in DFS or OS was observed between patients with HER2-zero or HER2-low tumors regardless of HR status [43]. Sato et al. reported that the OS was significantly better in HER2-low than in HER2-negative patients. However, multivariate logistic regression analyses showed that HER2-low status was not an independent factor for OS [28]. Another study demonstrated that HER2-low breast cancer patients had better DFS, OS, and BCSS in comparison with HER2-0 cases. Notably, survival outcomes varied by menopausal status: BCSS benefited premenopausal patients, while DFS and OS showed greater benefits for postmenopausal patients [44].
In a study by Liu et al., the HER2-0 group exhibited superior DFS compared to the HER2-low group across the entire population (p = 0.003), as well as lymph node-negative (p = 0.009) and HR-positive (p = 0.007) subgroups. Multivariate regression analysis revealed that low HER2 expression was an independent negative prognostic factor for DFS in the HER2-negative population with early-stage breast cancer (HR = 1.33; 95% CI: 1.06–1.66; p = 0.013). The differences in DFS observed in the overall, lymph node-negative and HR positive subgroups indicate that HER2-low status may serve as a poorer prognostic indicator for disease progression in early-stage breast cancer [15]. Many studies evaluating the prognostic value of HER2-low expression in breast cancer, both in early-stage and metastatic disease, have not identified a significant difference in OS between HER2-low and HER2-0 tumors [12, 14, 19, 37, 45]. Therefore, the Expert Consensus Statements by the European Society for Medical Oncology (ESMO) suggest that the prognostic value of HER2-low expression (IHC 1+ or 2+/ISH-negative) remains insufficient [36].
In our study, no significant difference in OS was found between subjects with HER2-low status and HER2-zero. However, subgroup analysis showed that patients with ER-negative receptor status (ER-) and HER2-low status had worse OS worse compared to those with the HER2-zero status and ER negative receptor status. Additionally, non-significantly worse OS was noted in HER2-low status patients with higher tumor stages (T3-4) and higher histological grades (G3). There were no differences in OS between subjects with HER2-low1+ tumors and those with HER2-low 2+/(ISH-) tumors.
In conclusion, HER2-low status was associated with HR positivity. Both subgroups of HER2-low tumors (HER2-low1+ vs. HER2-low IHC 2+ with negative ISH) exhibited positive HR receptor status. CHEK2 pathogenic or likely pathogenic variants were found in patients with HER2-low2+/ISH(-) status. There was no significant association between the HER2-low subgroups (HER2-low1+ vs. HER2-low IHC 2+ with negative ISH) and factors such as BRCA gene mutations, tumor size, N+, G, and hormone receptor status. However, HER2-low status was associated with worse OS in subgroups of patients with negative prognostic factors compared to patients with HER2-zero status. Specifically, HER2-low1+ status was associated with worse OS in subgroups with negative prognostic factors, such as G3, T3-T4, PR-, and HR-, compared to patients with HER2-low2+/ISH(-) tumors.